Navigation
The Four Tool Boxes for Class II Treatment
Informed consent is the legal responsibility of the orthodontist to explain the pros and cons of all possible treatment options and to help the patient and their family determine which option is best for them.
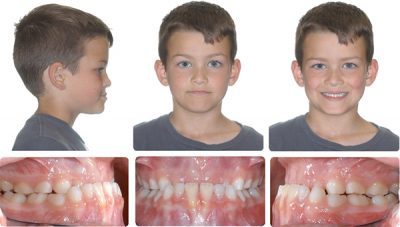
One type of Class II bite problem is when there is a horizontal gap between the upper and lower front teeth, also known as excess overjet. 53% of the population has a Class II bite with an overjet greater than 3mm. 15% of the population has a moderate to severe Class II bite problem with 5mm or more of overjet.
The cause of excess overjet is usually a small or receding lower jaw and chin, but there can also be a protrusion of the upper front teeth.
Xbow System Lectures
The Four Tool Boxes for Class II Treatment
The Four Tool Boxes for Class II Treatment
Informed consent is the legal responsibility of the orthodontist to explain the pros and cons of all possible treatment options and to help the patient and their family determine which option is best for them.
One type of Class II bite problem is when there is a horizontal gap between the upper and lower front teeth, also known as excess overjet. 53% of the population has a Class II bite with an overjet greater than 3mm. 15% of the population has a moderate to severe Class II bite problem with 5mm or more of overjet.
The cause of excess overjet is usually a small or receding lower jaw and chin, but there can also be a protrusion of the upper front teeth.
The Four Tool Boxes Analogy
Dr. Higgins’ office has four different options for treating a Class II bite problem.
- The Surgery Tool Box
Braces to straighten the teeth and place the front teeth and lips in an ideal position, followed by surgery to lengthen the lower jaw, is often the best option to correct the bite and balance the appearance of the nose, lips, and chin. - The Traditional Treatment Tool Box
Braces and the extraction of two upper teeth are used to retract or “pull back” the upper front teeth to correct the bite and camouflage the small or receding lower jaw and chin. We call this Class II compensation. This is a good choice if the upper front teeth are crowded or protruding. The downside of this treatment is that it can result in the loss of upper lip fullness. - The Crossbow Tool Box
The Crossbow Class II Corrector shares the correction between the upper and lower teeth. It moves upper teeth back and lower teeth forward. This minimizes the retraction of the upper front teeth and upper lip. This is another type of Class II compensation. It is meant to be used in a growing patient and works best if the patient has a growth spurt. The downside is that it still moves the upper lip back, just not as much as traditional extraction treatment. It also moves the lower lip forward, a plus or a minus. Even if surgery is the best option, most patients still choose the Crossbow Tool Box to avoid surgery and extractions. Sometimes, the Crossbow is not a good option, especially if the patient is finished growing, if the lower front teeth are crowded or protruded, or if the lower lip protruded. - The Class II Elastic Tool Box
Combined with Class II elastics, braces or Aligners are probably the most common treatments today. It is popular because it is the least expensive. It requires the least effort by the orthodontist, but the most effort by the patient. If the patient does not wear the elastics, they end up with straight teeth but with a remaining bite problem or excess overjet.
If the patient wears the elastics well, the result may be similar to the Crossbow, with two exceptions. Class II elastics tend to pull the upper front teeth down, making a gummy smile worse. Two, when used with aligners, Class II elastics may push the lower front teeth out of the bone, exposing the roots. The other problem with aligners is they require much more patient cooperation than braces, and there are many tooth movements that aligners don’t do well or not at all.
This is why the best orthodontists using aligners use them with braces. Braces are still used to do the “heavy lifting.”The general rule is it is best to choose a treatment plan that decreases elastic wear and patient cooperation because poor cooperation can increase the length of treatment. Long treatment time increases the risk of root resorption (root shortening) and decalcification (white spot lesions or cavities).
Dr. Higgins has developed systems that decrease the time in braces to 12 to 18 months, even for extraction treatment. This includes indirect (precision) bonding of brackets (braces). He also uses a low-force technique with a smaller bracket slot and smaller wires than most orthodontists. This is more comfortable for the patients and may result in less root resorption.
The Crossbow appliance is part of Dr. Higgins’ “foundation building” treatment philosophy. It is based on waiting until all teeth have erupted, including second molars, before placing full braces. “Building the foundation” includes establishing a normal upper jaw width with an expander (RME), correcting a Class II bite with a Crossbow appliance, and opening space for upper canine teeth with partial braces (RME X 6).
Dr. Higgins is a clinical assistant professor at the University of British Columbia. More information can be found on the Crossbow website at www.crossboworthodontic.com.
The Four Tool Boxes Analogy
The Crossbow Tool Box
The Crossbow Tool Box
The Crossbow Class II Corrector shares the correction between the upper and lower teeth. It moves upper teeth back and lower teeth forward. This minimizes the retraction of the upper front teeth and upper lip. This is another type of Class II compensation. It is meant to be used in a growing patient and works best if the patient has a growth spurt.
The downside is that it still moves the upper lip back, just not as much as traditional extraction treatment. It also moves the lower lip forward, a plus or a minus. Even if surgery is the best option, most patients still choose the Crossbow Tool Box to avoid surgery and extractions. Sometimes, the Crossbow is not a good option, especially if the patient is finished growing, if the lower front teeth are crowded or protruded, or if the lower lip protruded.
The Traditional Treatment Tool Box
The Traditional Treatment Tool Box
Braces and the extraction of two upper teeth are used to retract or “pull back” the upper front teeth to correct the bite and camouflage the small or receding lower jaw and chin. We call this Class II compensation. This is a good choice if the upper front teeth are crowded or protruding. The downside of this treatment is that it can result in the loss of upper lip fullness.
The Surgery Tool Box
The Surgery Tool Box
Braces to straighten the teeth and place the front teeth and lips in an ideal position, followed by surgery to lengthen the lower jaw, is often the best option to correct the bite and balance the appearance of the nose, lips, and chin.
The Four Tool Boxes Analogy
Dr. Higgins’ office has four different options for treating a Class II bite problem.
The Class II Elastic Tool Box
The Class II Elastic Tool Box
Combined with Class II elastics, braces or Aligners are probably the most common treatments today. It is popular because it is the least expensive. It requires the least effort by the orthodontist, but the most effort by the patient. If the patient does not wear the elastics, they end up with straight teeth but with a remaining bite problem or excess overjet.
If the patient wears the elastics well, the result may be similar to the Crossbow, with two exceptions. Class II elastics tend to pull the upper front teeth down, making a gummy smile worse. Two, when used with aligners, Class II elastics may push the lower front teeth out of the bone, exposing the roots. The other problem with aligners is they require much more patient cooperation than braces, and there are many tooth movements that aligners don’t do well or not at all.
This is why the best orthodontists using aligners use them with braces. Braces are still used to do the “heavy lifting.”The general rule is it is best to choose a treatment plan that decreases elastic wear and patient cooperation because poor cooperation can increase the length of treatment. Long treatment time increases the risk of root resorption (root shortening) and decalcification (white spot lesions or cavities).
Dr. Higgins has developed systems that decrease the time in braces to 12 to 18 months, even for extraction treatment. This includes indirect (precision) bonding of brackets (braces). He also uses a low-force technique with a smaller bracket slot and smaller wires than most orthodontists. This is more comfortable for the patients and may result in less root resorption.
The Crossbow appliance is part of Dr. Higgins’ “foundation building” treatment philosophy. It is based on waiting until all teeth have erupted, including second molars, before placing full braces. “Building the foundation” includes establishing a normal upper jaw width with an expander (RME), correcting a Class II bite with a Crossbow appliance, and opening space for upper canine teeth with partial braces (RME X 6).
Dr. Higgins is a clinical assistant professor at the University of British Columbia. More information can be found on the Crossbow website at www.crossboworthodontic.com.
The Class II Treatment Foundation
The Class II Treatment Foundation
Foundation Rules
- Treat the biggest problem first.
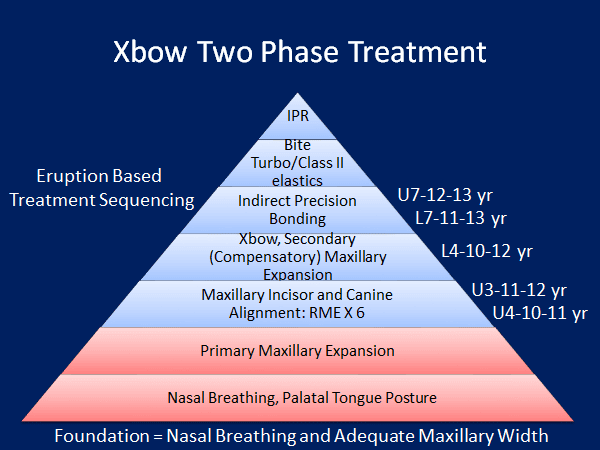
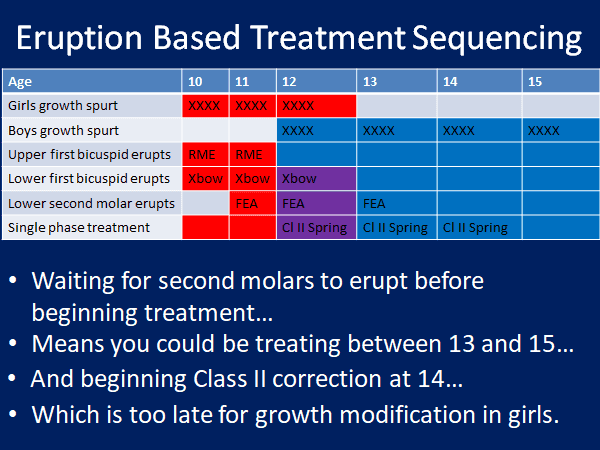
- Sequence treatment based on the eruption.
- Begin with primary maxillary expansion if a posterior crossbite or the maxillary lateral incisors are impacted. These teeth erupt at 8 to 9 years old on average.
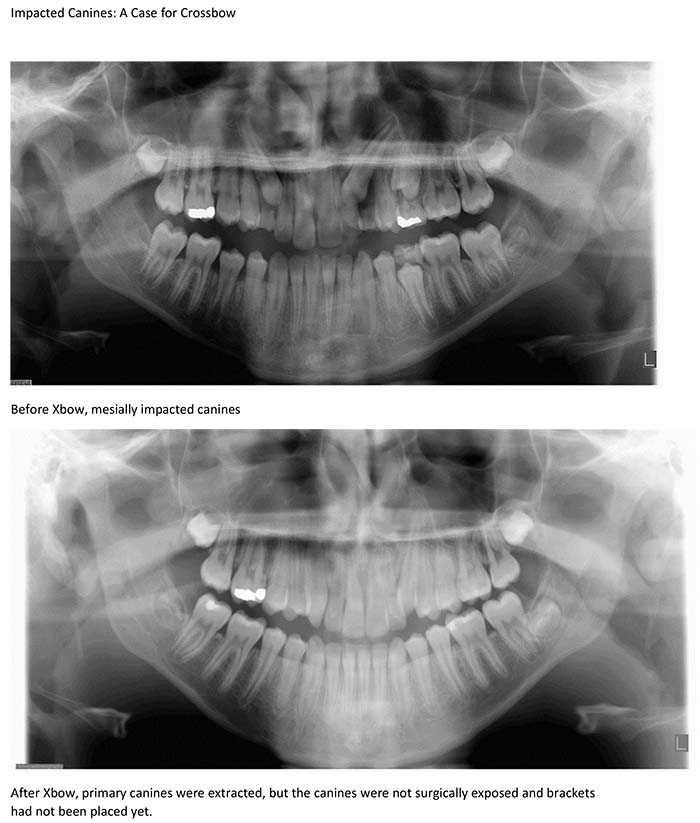
- Time first phase treatment when the first bicuspids erupt at 10 to 12 years old to make room for the erupting maxillary canines at 11 to 12 years. This will reduce the incidence of impacted maxillary canines.
- Don’t place full-edgewise appliances until the second molars erupt; you will prolong your second phase treatment and increase decalcification and root resorption.
- In deep overbite cases, save cooperation with Class II elastics until you are in full-size stainless steel archwires, and the overjet is reduced enough to place a bite turbo.
- Try to postpone the incisors’ IPR (interproximal reduction) until all spaces are closed, the buccal occlusion is Class I, and the overbite and overjet are corrected. The goal is to create long, flat interproximal contacts without black triangles, keeping in mind not to create a tooth mass discrepancy. This is impossible to do with early IPR.
- Always go back to the foundation base during treatment to ensure the patient can breathe through the nose, keep the tongue on the anterior palate, swallow without a tongue thrust, and keep the lips together at rest, if possible.

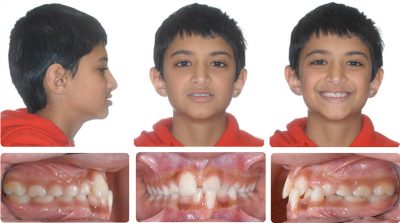
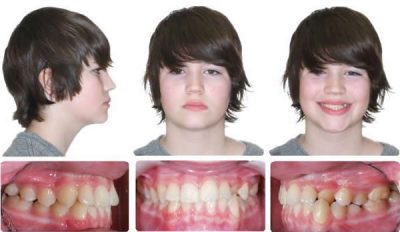
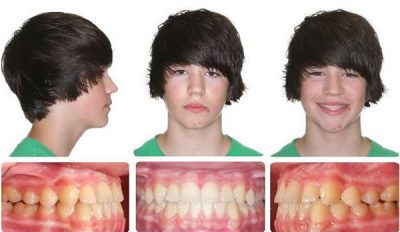
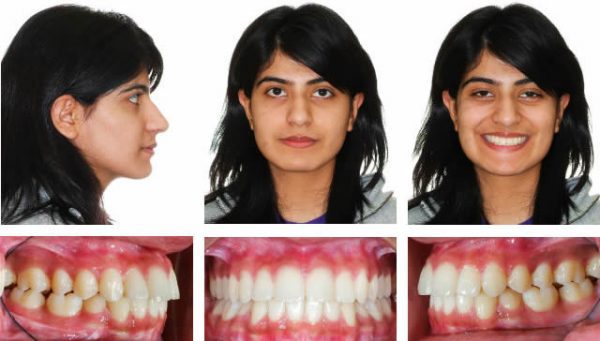
Initial, posterior Crossbite, and Anterior Crowding

4 Years After Maxillary Expansion
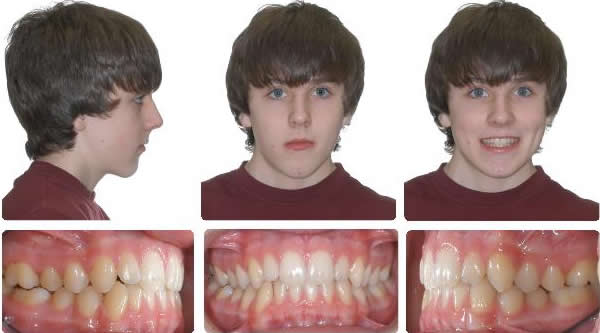
Taken 2 Years after Xbow Removal

Initial

4 Years After Maxillary Expansion

2 Years After Xbow, No Braces Used
RME X 6: Combining Maxillary Expansion and Anterior Alignment
RME X 6: Combining Maxillary Expansion and Anterior Alignment
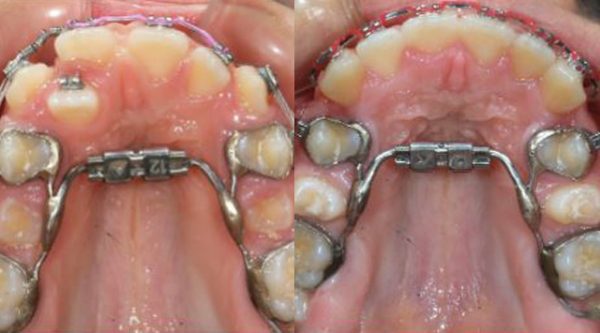
RME X 6: Combining Maxillary Expansion & Anterior Alignment to Establish the Maxillary Foundation. The Xbow System is based on treating to an ideal maxillary arch form and width. Combining anterior alignment with Rapid Maxillary Expansion is more effective than archwire expansion.

RME X 6 appliance with 12 mm Dentaurum “Variety” expansion screw, 100-gram shorty open coil nickel-titanium springs to open space for canines, occlusal rests for second molars. Mini tubes are welded to the first bicuspid bands in such a way as to control the movement of the canine and incisor occlusal plane.

After 6 Months RME X 6

RME X 4/Xbow with Mesial Hookup & Upper Incisor Segment


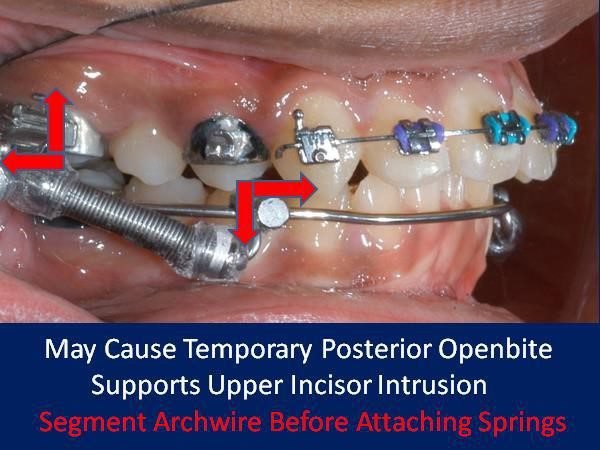
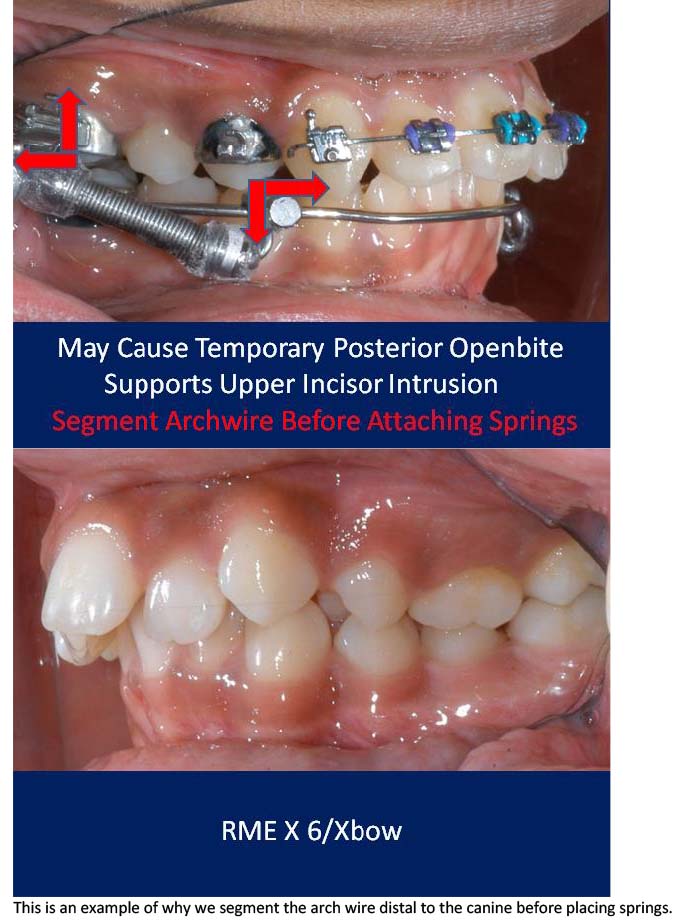
RME X 6/Xbow appliance with mesial hookup and archwire segmented distal to canines before Class II spring attachment.

RME X 6/Xbow after Class II springs were removed after over-correction of Class II, and the spring side effect of the buccal segment occlusal plane tipping down in front was shown. If the archwire had not been segmented, the anterior teeth would have been extruded and tipped lingually into crossbite.
RME X 6/Xbow Cases Treated by Dr. Higgins

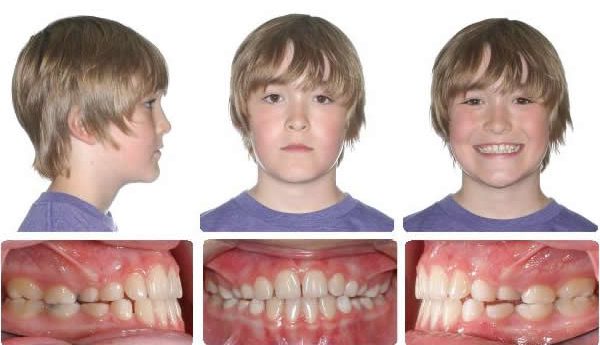
Initial

After Upper Incisor Alignment, Day of Xbow Insertion

Initial
- After Upper Incisor Alignment, Day of Xbow Insertion
- After 3 Months of Xbow Followed by Compensatory Maxillary Expansion, Now Retain Expansion & Test Class II Correction for 5 Months Before Removing Appliances
- Ready for Phase 2 Braces
- 8 Months Braces
This high-angle patient presented with a half-cusp Class II bicuspid relationship and a bicuspid open bite on the right side.
After RME X 6/Xbow Showing Buccal Segment Over-Correction. Once the Anteriors Were Aligned, the Triple “L” Arch & Springs Were Placed. The springs were on for three months before the compensatory maxillary expansion was started. The expansion was retained for five months before the appliance was removed.
After 3 Months of Xbow Followed by Compensatory Maxillary Expansion, Now Retain Expansion & Test Class II Correction for 5 Months Before Removing Appliances

Ready for Phase 2 Braces

8 Months Braces

This high angle patient presented with a half cusp Class II bicuspid relationship and a bicuspid openbite on the right side.

After RME X 6/Xbow Showing Buccal Segment Over-Correction. Once the Anteriors Were Aligned the Triple “L” Arch & Springs Were Placed. The springs were on for 3 months before compensatory maxillary expansion was started. The expansion was retained for 5 months before the appliance was removed.

10 Months Full Braces


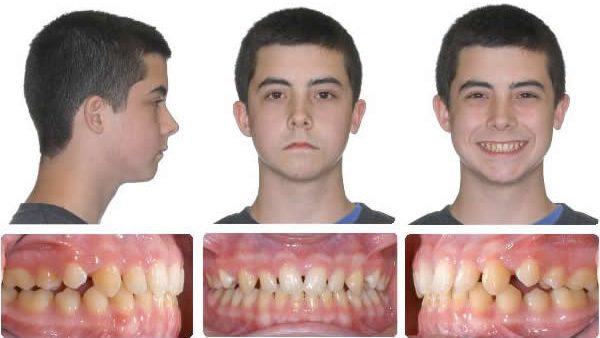
Initial

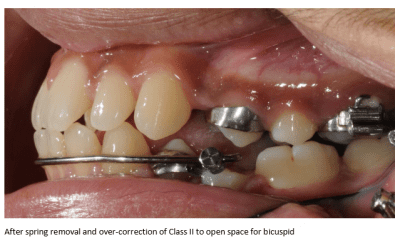
After upper alignment and Xbow correction to Class I bicuspid. Leave springs on to over-correct.

Day of spring removal after over-correction. Springs were on for 4 months.
RME X 6 with upper second molar mini tubes on bicuspid bands. 016X.025 SS anterior segment (Use active retraction of upper incisors with a continuous archwire as little as possible to avoid root resorption.)

Day of appliance removal and placement of upper Essix retainer, Ready for indirect bonding of full braces.

7 Months Full Braces

Initial

RME X 6v-v2. 4 Months Xbow, Ready for Maxillary Expansion

11 Months After Spring Removal, Full Braces Have Not Been Used
Class III Malocclusion
The RME X 6 is used with Class III malocclusions when maxillary expansion and upper incisor proclination is indicated. A reverse pull headgear (protraction face mask) can be added by attaching elastics to the first bicuspid hooks or the long ends of the archwire distal to the bicuspid tubes.


Progress


RME will open space for upper lateral incisors. RME X 4 and bonded posterior bite blocks to rotate mandible down and back and then procline upper incisors.
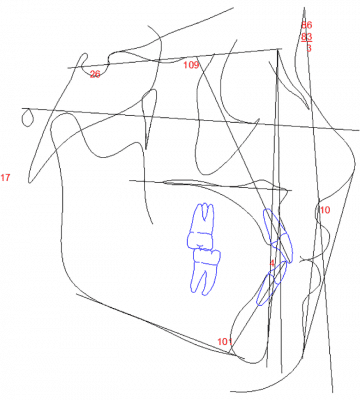
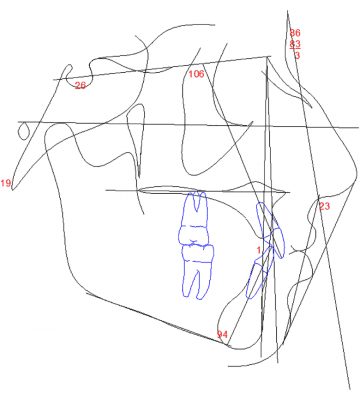
Class II Compensation Compared to Class III Compensation
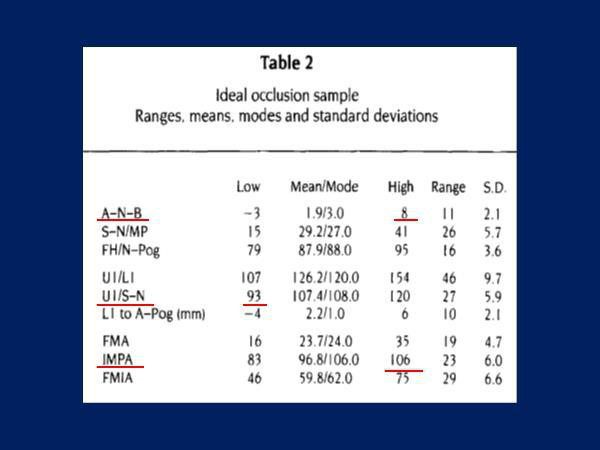
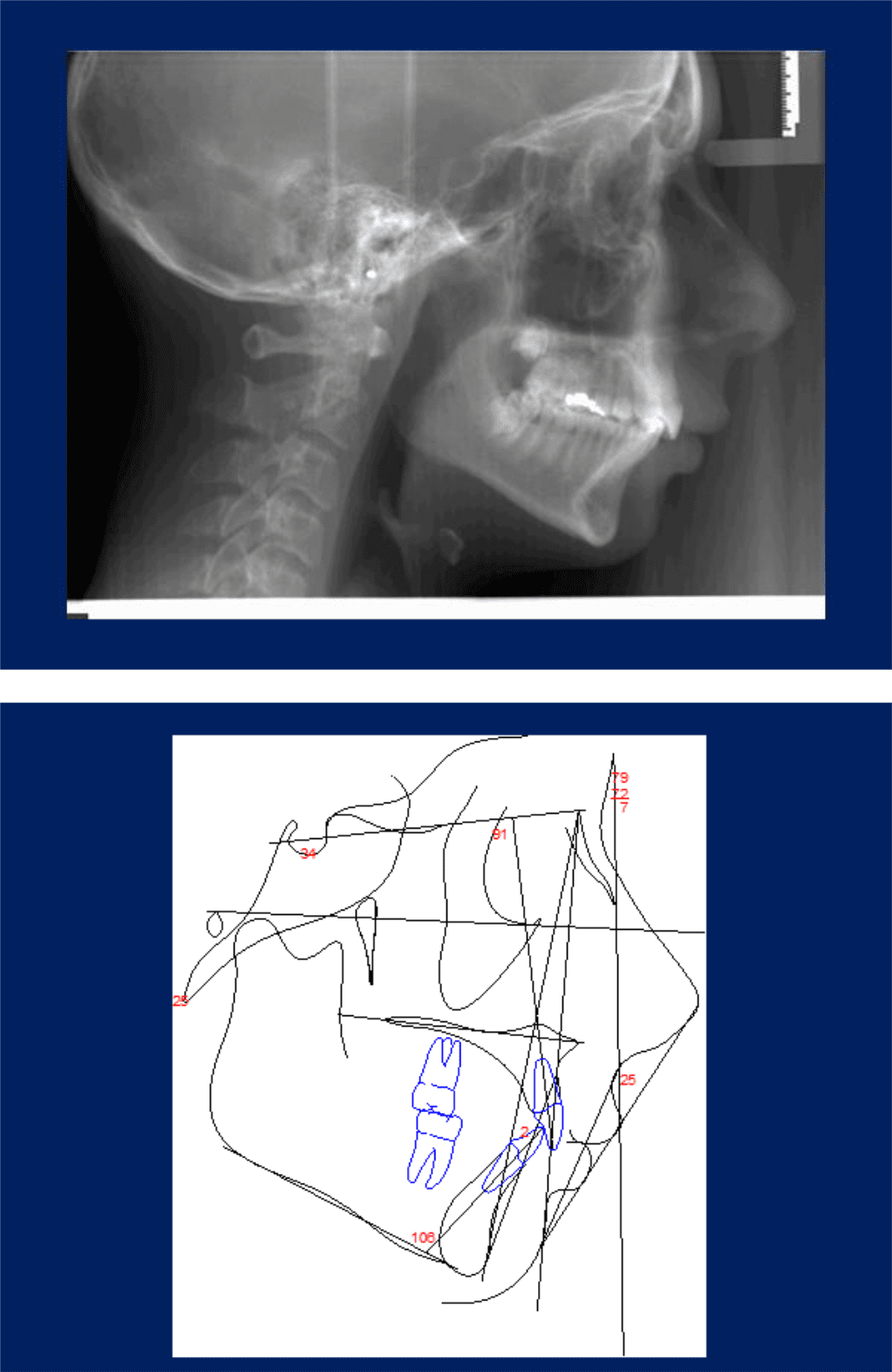
In Dr. Casko’s untreated ideal occlusion study, where the ANB angle was -3 degrees, the lower incisor was compensated back to 83 degrees while the upper incisor was compensated out to 120 degrees. To prevent Class III surgery, orthodontists will procline upper incisors out to 120 degrees without a second thought, which is 18 degrees past the norm. The same orthodontists may criticize a lower incisor proclined to 106 degrees in a Class II patient, which is only 10 degrees past the norm.
The same patient as above flipped lower to upper. Why should a Class II be treated differently than a Class III?




Proclining Upper Incisors to Avoid Cl III Surgery



Initial
Progress
Final

Maxillary expansion and protraction headgear for four months, followed by two months of settling.


Initial


Initial

6 Months maxillary expansion and protraction facemask, photos taken one month after appliance removal, note mandibular asymmetry, Class II right, Class III left.

RME & Protraction Facemask
After 6 Months RME X 6
10 Months Full Braces

Progress
End of Phase One
- Initial
- Progress
- Final
- X-Rays
Initial to Final
Maxillary expansion only opens space for the upper lateral incisors, and the mandible is rotated down and back, correcting the anterior crossbite.
9 Months Braces
Initial
(CAAPP) Orthodontic Skating: Sliding with Control
(CAAPP) Orthodontic Skating: Sliding with Control

CAAPP with G&H Agility PSL brackets on canines and bicuspids.
Combination Active Anteriors and Passive Posteriors (CAAPP) Orthodontic Skating: Sliding with Control
CAAPP with G&H Agility PSL brackets on canines and bicuspids.
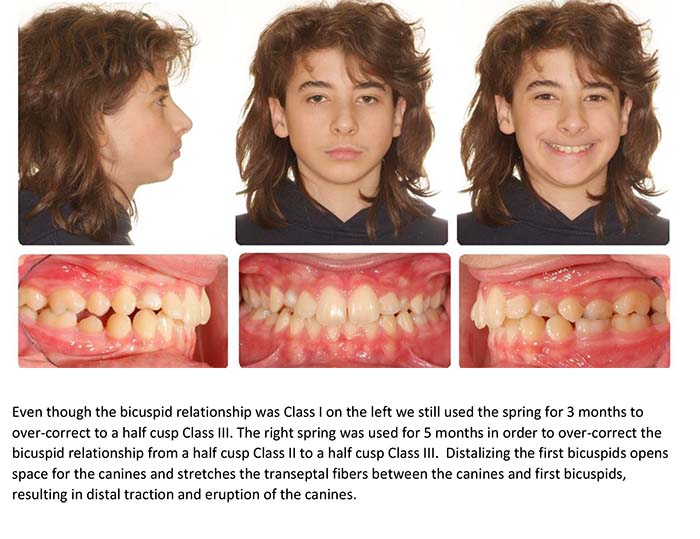
CAAPP combines incisor control with ligated twin brackets and decreased resistance to sliding with passive self-ligating brackets on canines and bicuspids, creating a “long buccal tube.” Ligated incisors also give young patients what they ask for, such as colored ligatures.
.018 inch bracket slot, .018X.025 inch archwire, Carriere passive self-ligating bracket sliding on archwire with Innovation active self-ligating brackets acting as end stops.
.018 inch bracket slot, .016X.022 inch archwire, Lotus Plus passive self-ligating bracket sliding on archwire with Lotus Plus interactive self-ligating brackets acting as end stops.
In a group of 145 consecutively debonded patients from the author’s practice, the average treatment time from bonding to debonding was 16 months. 78% of the patients had an average treatment time of 13.4 months.
The part of treatment that the orthodontist has control over (other than the treatment plan) is Alignment and Space Closure (ASC). The patient controls elastic wear to coordinate the arches and finish the occlusion. In a group of 42 consecutively treated patients, where 34 were non-extraction, and 8 were extraction cases, ASC took an average of 9 months to complete for the non-extraction group and 11 months for the extraction group.
CAAPP TwinLok 1997
I was asked to test the .018 version of the TwinLok passive self-ligating bracket in 1997. The result was the incomplete alignment of the lower incisors and a lack of torque control of the upper incisors. This was due to the play between the archwire and the slot. The slot depth was .030 inches. This was done to accommodate the anterior curvature of the archwire and still allow the clips to close.
The low resistance to sliding in the canine and bicuspid brackets was an advantage. It was easier to close space, retract canines, and advance incisors.
I changed the TwinLok brackets to ligated twins on the incisors and traded free sliding for control, creating a hybrid system similar to Dr. Gianelly’s bi-metric technique.
Ligating the archwire to the incisor bracket slots’ base allows the maximum deflection and activation of the lightest archwires and the fastest incisor alignment with the lightest forces.
Proponents of passive self-ligating brackets thought that ligated incisor brackets would slow down anterior alignment and require heavier forces to overcome resistance to sliding. The following examples show that this is not the case.



Initial




The following is a bicuspid extraction case showing rapid alignment with CAAPP.

Initial




I am using the Lotus Plus DS Hybrid self-ligating bracket system, which is active on incisors and passive on canines and bicuspids. I use the MBT prescription in a .018-inch slot. The slot tolerances are tight, and we sometimes find it difficult to close the clips when using .017X.025-inch archwires.
Presently, the archwire progression we are using is .012-inch niti, followed by .014-inch niti (if necessary), followed by .018-inch niti to the second molars, followed by .016X.022-inch niti, and finally, .017X.022-inch heat-treated stainless-steel archwires. Final adjustments are done in .016X.022-inch beta titanium.
When I started with Dr. Michael Wainwright, he used two archwires, a .016-inch Niti followed by .016X.022-inch stainless steel. I was amazed at the simplicity and efficiency compared to the segmented arch technique that we were both taught at Indiana University. I am now using more archwires in the progression, but I am convinced I am using the lightest forces, decreasing root resorption and making it more comfortable for my patients.


The Lotus Interactive Niti clip seats the archwire in the slot’s floor with a force perpendicular to the slot, unlike a “C” Clip.

Four arch sizes=three pairs (Small, Medium, Large)
To purchase these wires in most sizes contact Mark James at G and H Orthodontics.
The Class II Compensation Compromise: Preserving the Upper Lip
The Class II Compensation Compromise: Preserving the Upper Lip




Before

After, treated non-extraction with phase one bionator followed by full edgewise and cervical headgear, care taken not to procline lower incisors.

Same patient showing opening of naso-labial angle due to upper incisor retraction.
This patient was the one that made me think more about preserving the upper lip. I read everything I could find in the orthodontic, surgery, and periodontal literature. My study club invited Dr. Clark to speak to us about Twin Blocks. I began using Twin Blocks but changed to the four crown cantilever Herbst appliance. The temporary over-proclination of lower incisors surprised me at first, but I did not see a gingival recession. Sharing the correction between the upper and lower resulted in less upper incisor and upper lip retraction.
As an orthodontic student in 1979 we were taught that our tool for a Class II malocclusion was orthodontic retraction and every problem was a protrusion.
Our toolbox had headgear and upper bicuspid extraction in it. In an emergency we could pull the red handle and use Class II elastics, but only if the lower incisors were retroclined or if we also extracted lower bicuspids. We looked at the models and the hard tissue ceph measurements.
For years I have been looking at the face as the most important determinant of which treatment I should recommend. For Class II patients this often means I will recommend jaw surgery as the best treatment. If the patient declines surgery I tell them treatment will involve dental compensation for their underlying jaw problem and that a compromise will involve a certain amount of upper incisor and upper lip retraction.
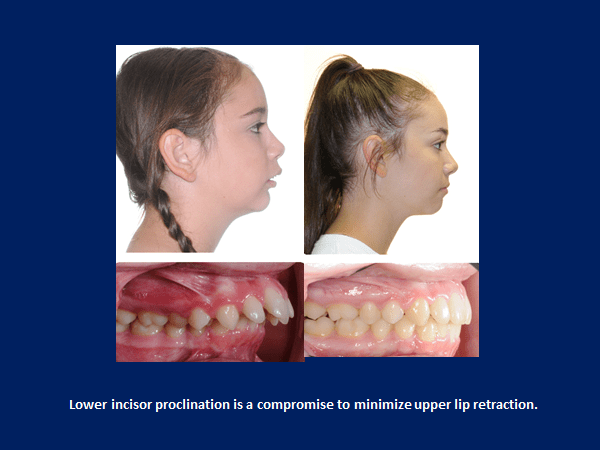
To minimize the retraction, Xbow shares the correction with the lower arch. This means lower incisor proclination and pemanent retention.
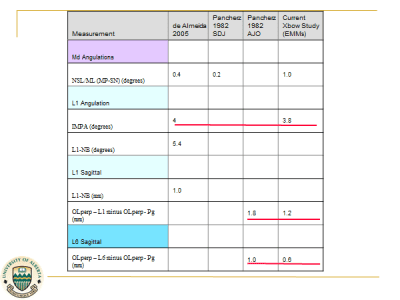
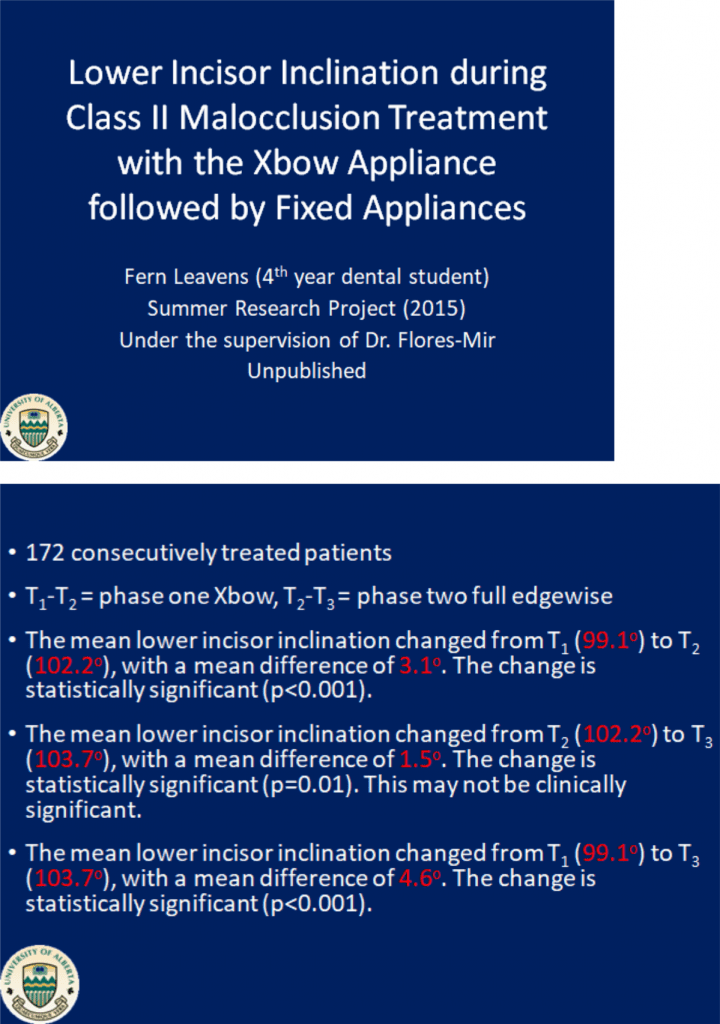
Xbow proclines lower incisors 3 degrees on average after a short period of over-proclination and rebound uprighting. In an unpublished study at the U of Alberta on 172 consecutively treated Xbow patients, the average lower incisor started at 99 degrees and ended up at 102.
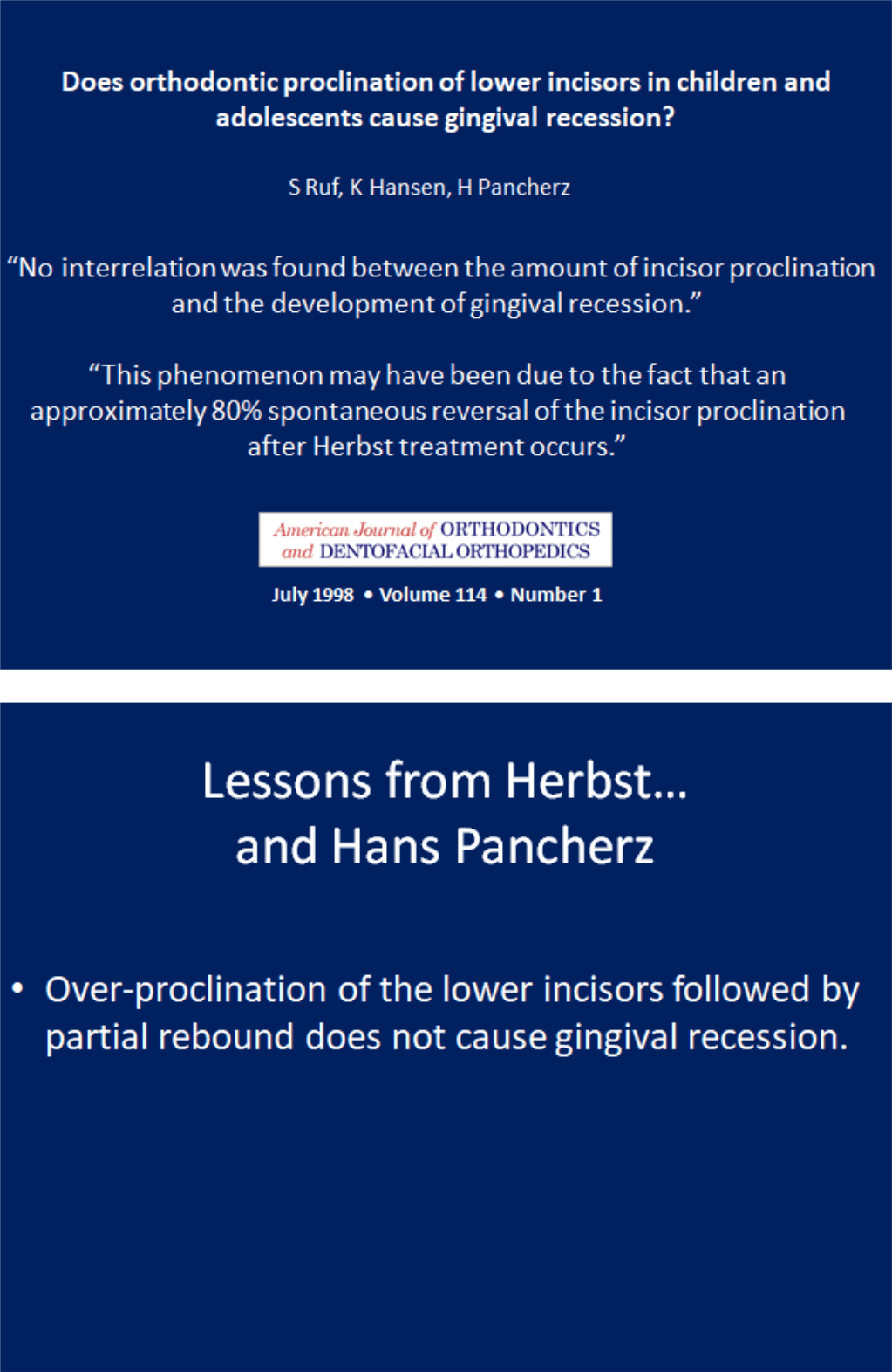
The literature is very clear. Lower incisor proclination does not cause gingival recession in healthy periodontium.
The literature is also very clear that all inter-arch Class II appliances procline the lower incisors a similar amount, even functional appliances. The non-edgewise Herbst appliance is capable of temporary over-proclination of the lower incisors similar to Xbow. This same over-correction is why the results are stable, and why phase two is shorter.


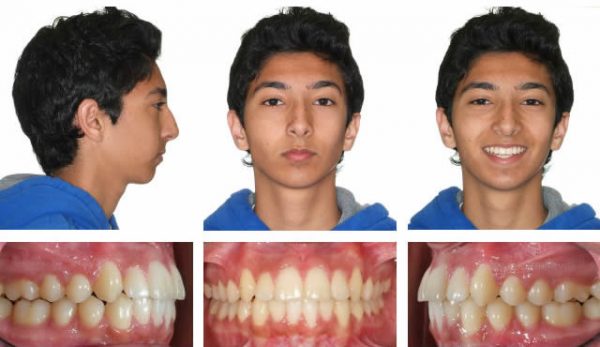
The Xbow system for Class II compensation is based on building the maxillary foundation for ideal treatment as if we were proceeding with jaw surgery. After maxillary expansion and upper anterior alignment, instead of proceeding with full braces and jaw surgery, we use the Xbow appliance to share the correction between both arches to minimize retracting the upper incisors and upper lip, compared to headgear or upper extractions.
















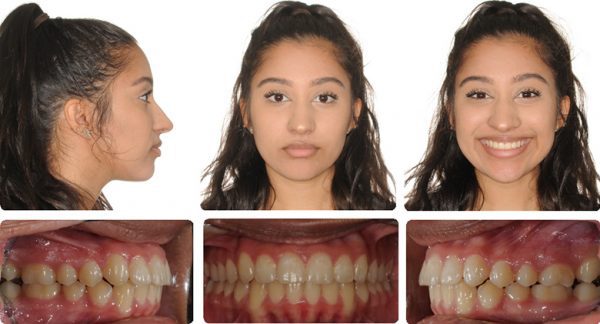
This case is an example of non-extraction treatment in a Class II crowded deep overbite malocclusion with a convex profile.











The goal should be to maintain the upper incisor position. If this is not possible it is better to end up with a slight protrusion and long-term retention instead of a retrusion based on the wishful thinking of better stability. We cannot predict how much more nasal growth will occur, only that it will.
More Compromises
This is a common conversation I have with orthodontists that criticize Crossbow. It starts by an orthodontist saying he uses headgear to prevent lower incisor proclination. I ask what if the patient doesn’t wear the headgear? The orthodontist will reply that they will add Class II elastics. I add that will procline lower incisors. They reply that they use a full size wire and -6 degree lower incisor brackets to prevent the lower arch from coming forward. (Myth) I ask what if the patient doesn’t wear the elastics. They reply that is when they place Forsus Springs. I add that will push the lower arch forward. They reply not if they use a full size wire and -6 degree lower incisor brackets. (Myth)
I ask what if they see side effects like posterior openbite, upper molar flaring, or occlusal plane canting. They reply they add vertical elastics. I thought they wouldn’t wear elastics. They reply the result will be a compromise:)
Lower incisor proclination is not ideal, but neither is orthodontic compensation when the ideal treatment is jaw surgery. Sometimes we get lucky and the patient and parents agree to ideal treatment. Sometimes we compromise.
The Debate Over Lower Incisor Proclination and Gingival Recession
Read MoreCrossbow’s Competition: Dealing With Side Effects
Read MoreThe Debate Over Lower Incisor Proclination and Gingival Recession
The Debate Over Lower Incisor Proclination and Gingival Recession
Part 1: Introduction
When I was an orthodontic resident in 1979, we were taught how to treat an upright lower incisor. The only expansion allowed was a sutural expansion with an RME. The “shared belief” was that lower incisor proclination would result in gingival recession. In the 1980s, my Class II patients fell into four groups.
- Orthodontic decompensation and jaw surgery,
- Two-phase non-extraction beginning with a functional appliance (which evolved into Herbst followed by Xbow),
- One phase four bicuspid extraction and headgear,
- One phase upper bicuspid extraction.
One thing became clear. If I extracted four bicuspids in a deep overbite case, I chased the lower incisors in what I call the “never-ending overjet.” In these cases, I saw the most lip retraction or profile flattening. I began treating more and more of these non-extraction cases in two phases.
No matter which interarch Class II appliance I used, I proclined lower incisors. Whether it was Xbow or Herbst or Twin Block or Class II elastics or Forsus, it didn’t matter. Expand buccally? Interproximal reduction?
Fill the slot and tie it back. Minus six-degree lower incisor brackets? They still proclined. I didn’t worry about proclining lower incisors with functional appliances until I began using Herbst.
(So this is what happens with full-time wear.) Even then, I didn’t see any gingival recession, which agrees with the article by Hans Pancherz and a systematic review on proclination. I am more comfortable with lower incisor tipping followed by partial uprighting with Xbow and non-edgewise Herbst than I am with bodily mesialization with a rectangular archwire and minus six degrees lower incisor brackets, which I find results in root prominence.
Dr. Anthony Mair explains it this way: “It is better to tip the crown and leave the root in bone than to bodily move the root out of bone; this setup is more reflective of natural compensation“
Dr. Mair has recently reported on several cases where Class II elastics used against a lower aligner caused bony dehiscence due to bodily movement of the lower incisors. The solution was to torque the root apex back into the alveolar bone as recommended by Dr. Laursen et al. (Am J Orthod Dentofacial Orthop 2020;157:29-34)
Dr. Mair warned that we should prepare for more of these cases as the popularity of Class II elastics used with aligners increases.
Part 2: The history involving my 40 years as an orthodontist
1979-1981: I was an orthodontic resident at Indiana University. Class II’s were treated by bicuspid extraction and headgear. Class II elastics were discouraged. We heard Drs. Rocke and Kesling speak on treating non-extraction with Class II elastics. They showed ceph tracings similar to what other orthodontists achieved with functional appliances such as activators, bionators, and Frankel appliances. It combined skeletal and dental effects, including lower incisor proclination.
Dr. Ricketts impacted our profession by introducing soft tissue analysis and the “Esthetic Plane.” He said that over-extracting could be detrimental to the face. He suggested that lower crowding in a deep bite was related to the lower arch being contained by a constricted upper arch.
The lower incisor tends to be more proclined in low mandibular plane angle cases with a normal overbite and more upright in high mandibular plane angle cases with a normal overbite. Dr. Ricketts taught that four bicuspid extractions should be done more in high-angle cases with a shallow overbite. Low-angle cases with deep overbite should be treated non-extraction.
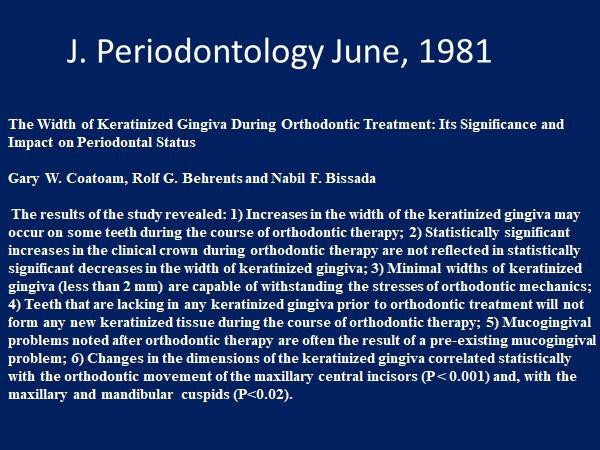
1981: Dr. Behrents published a groundbreaking article in the Journal of Periodontology that was the first to debunk myths that I had been taught. 1981-1984: I was an associate with my mentor, Dr. Michael Wainwright. He taught me indirect bonding, two-phase treatment, and combined orthodontic/orthognathic surgical treatment.

1984: I opened my office in North Delta. I began using functional appliances. I took a ceph at the final records. I was proclining lower incisors with the functional appliances, but I was not seeing gingival recession. This became a subject that would interest me for my entire career. Dr. Casko published his findings that questioned Tweed’s 95-degree IMPA in untreated Class II skeletal patterns with Class I occlusions. More myth debunking.
Dr. Casko believed that incisor inclination was linked to the skeletal pattern and showed that it was normal for the lower incisor to have an IMPA higher than 95 degrees in an untreated skeletal Class II with a Class I occlusion. He argued that this should be the goal for Class II compensation.
Example from my practice:
Naturally occurring Class II skeletal with Class I dental and a retroclined upper incisor and proclined lower incisor. Dr. Creekmore agreed with Dr. Casko.

1990: My study club invited Dr. William Clark to discuss twin blocks. I began using them.
1991: Dr. DeVincenzo published his research, which is the first of many to question the ability of functional appliances to increase mandibular length in the long term. Dr. Lysle Johnston coined the term “mortgaging mandibular growth.”
More myth debunking.

1995: I began using the four-crown Herbst appliance, which made me interested in non-compliance appliances.
My main concern was over-correction; I saw a noticeable lower incisor proclination that I had not noticed with removable functional appliances. I tried placing -5 to -10 degree lower incisor brackets, but instead of proclining the lower incisors, I noticed that the bodily mesialization of the incisors resulted in a “washboard effect.” I preferred tipping the lower incisors temporarily and then allowing them to upright before phase two.
The important thing was that I did not see the gingival recession I had been taught would happen.
Dr. Alan Lowe developed the Klearway appliance for snoring and sleep apnea. Long-term wear has resulted in severe proclination of lower incisors without a significant recession.
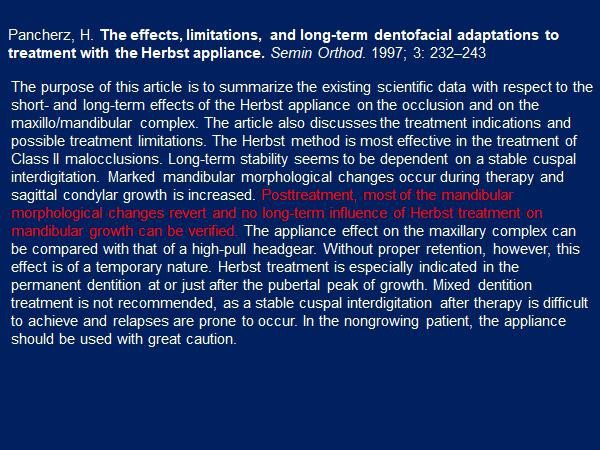
1997: Dr. Pancherz published his summary of the effects of the Herbst appliance. There was no long-term increase in mandibular length. He did not recommend it in non-growing patients, possibly due to the risk of condylar resorption, which he had shown.
(Dr. Woodside also showed condylar resorption with the Herbst appliance. When I lectured at the University of Toronto, Dr. Woodside commented that the Crossbow Appliance was probably kinder to the condyle than the Herbst appliance because the springs were stress breakers and allowed the condyle to function in the fossa.)
The takeaway message was that mixed dentition treatment was not recommended because “a stable cuspal interdigitation after therapy is difficult to achieve, and relapses are prone to occur.” Pancherz had proven what Dr. Herbst called “the bite-catching effect.”

Thanks to Dr. Herb Hughes for the above slide showing over-correction with Xbow and the bite-catching effect of the steep cuspal inclines of the first bicuspids.
1998: Dr. Jay Bowman published an article in the JCO using Jasper Jumpers attached to a lower lip bumper instead of a bypass. I was convinced that most Class II’s required maxillary expansion. I also used lower lingual arches to preserve the “e” space. I added a lip bumper and Ormco’s Bite Fixer springs. This led to the Xbow appliance. Dr. Pancherz publishes his findings on the Herbst appliance and gingival recession.
2000: Dr. Gianelly gives us a target to shoot for.
2001: Granted a US patent and registered trademarks for the Xbow
2002: I lectured on the Xbow appliance with Dr. Pancherz at the GLAO/MASO meeting. We discussed lower incisor proclination and agreed that temporary over-proclination followed by uprighting did not cause a gingival recession. Over-correction followed by the bite-catching effect and cuspal interdigitation was necessary for long-term stability.
2009: First Xbow research paper published in the AJODO after working with Dr. Carlos Flores-Mir at the U of Alberta.
We showed the lower incisor proclined a similar amount to the Herbst appliance. A total of seven papers on Xbow would be published as a result of Dr. Flores-Mir’s effort
2013: Drs. Bob Miller and Carlos Flores-Mir published the definitive research paper on the efficiency of the two-phase Xbow treatment compared to the one-phase Forsus to the archwire treatment.

2015: The data from 172 consecutively treated Xbow patients was studied at the U of Alberta. An interesting finding was that the average initial lower incisor inclination was 99 degrees. This agrees with Dr. Casko’s belief that Class II skeletal cases are naturally compensated.
2016: I was asked to speak at the AAO Scientific Session. I concluded that the results are similar for all inter-arch Class II appliances. The differences are probably not clinically significant. We should focus on preserving the upper lip and treatment efficiency, including decreasing the treatment time for full-edgewise appliances.
2017: Dr. Gianelly’s 76% non-extraction target looks right on.
The eye-opener:
2019:
These are some heavy hitters in our profession. Dr. Buschang’s research has shown little evidence to prove that lower incisor proclination causes gingival recession. Dr. Behrents told us in 1981 that some recessions were normal and that severe recessions could be prevented if an attached gingiva was present or a graft was placed before ortho.
Dr. Lindauer asked me to speak on Crossbow at the AAO in 2016.
Part 3: Ancient History
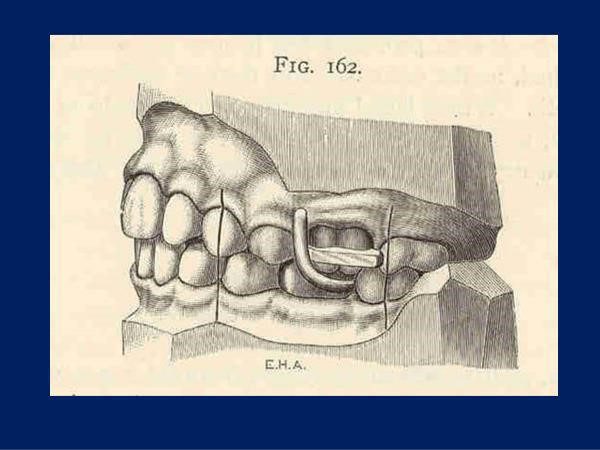
Dr. Angle’s Class II “bite-jumping” appliance, photo courtesy of Dr. Lysle Johnston. This would have resulted in lower incisor proclination. If this had caused gingival recession, Dr. Angle would have reported it.
Dr. Angle’s students, Begg and Tweed, stopped doing what they had been taught and followed the teachings of Calvin Case. Dr. Tweed could control the torque of the upper incisors as he retracted them to reduce the overjet in Class II’s. He could also level the Curve of Spee with full-size rectangular archwires and Class II elastics to erupt the lower posterior teeth.
When you look at the model, Tweed can make a Class II case look like an ideal Class I skeletal dental, complete with upright incisors. In 1930, Dr. Broadbent invented the cephalometer, which allowed Tweed to measure the inclination of the incisors and compare his results to those of untreated Class I dental-skeletal patients. This led to the Tweed Triangle and the goal of treating an upright lower incisor. Tweed was known for saying, “Put your plaster on the table,” but the cephalometric measurements gave scientific support to the upright lower incisor.
It wasn’t until 1956 that Tweeds’ results were studied closely by Drs. Stoner and Lindquist at Indiana University. Their study “Consecutive Cases Treated by Dr. Charles Tweed” was published in the Angle Orthodontist.
It looked at the claim that Tweed mechanics resulted in improved facial esthetics. The main finding was that overjet reduction was almost all by upper incisor retraction. I met Dr. Lindquist while I attended Indiana University. He was the first orthodontist that I heard warn of over-extracting. He said that serial extracting was a “self-fulfilling prophecy” in that extracting primary canines increased the odds that first bicuspids would need to be extracted. He advised only extracting lower primary canines if the lateral incisors were impacted or blocked.
Crossbow’s Competition: Dealing With Side Effects
Crossbow's Competition and Dealing With Side Effects

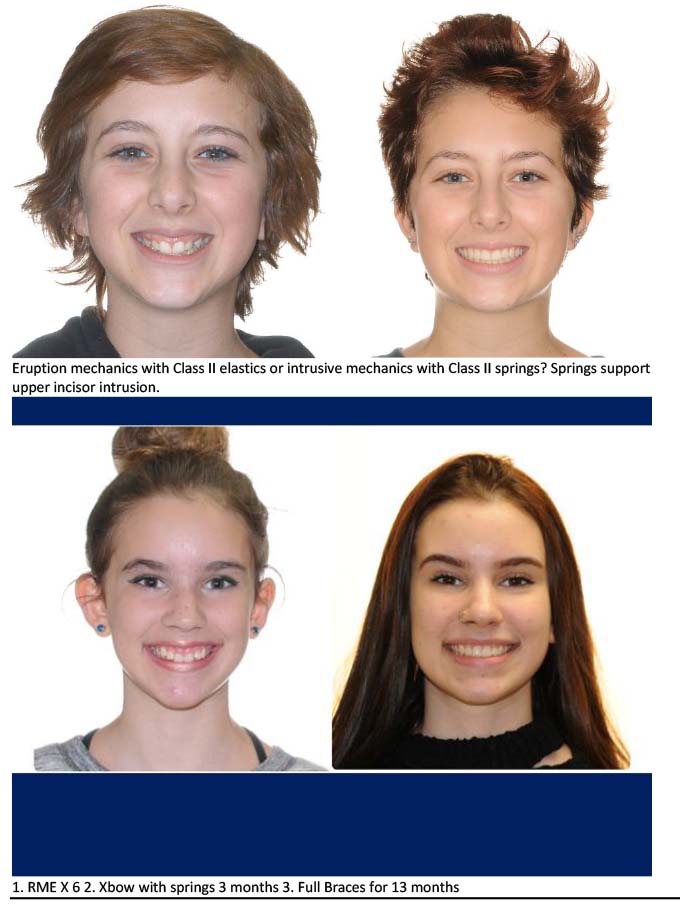
Bite opening in phase two with eruption mechanics (bite turbo and Class II elastics) while the patient is growing and mandibular growth can compensate for the downward and backward rotation of the mandible.


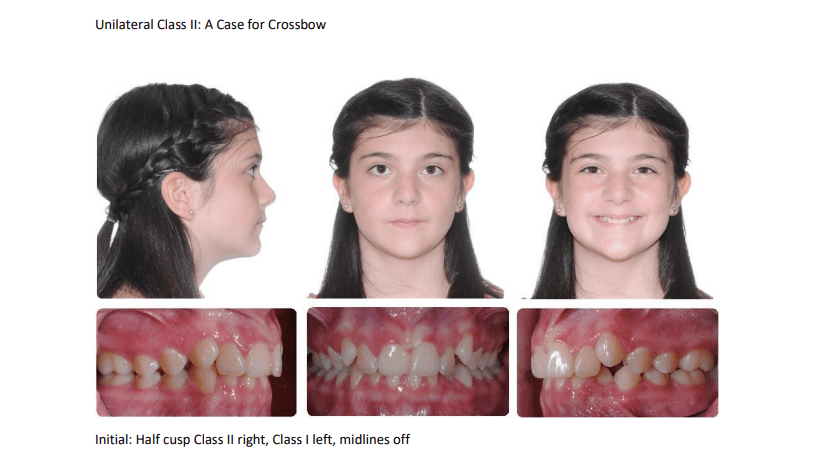
Initial unilateral Class II

Left spring only

Over-correction after 5 months, incisors edge to edge, note side effect of posterior openbite but no anterior occlusal canting

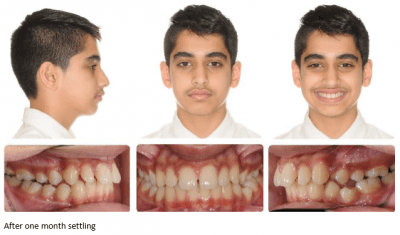
After 1 month settling

After 2 months settling

After 5 months settling

This is an example of why we segment the arch wire distal to the canine before placing springs.
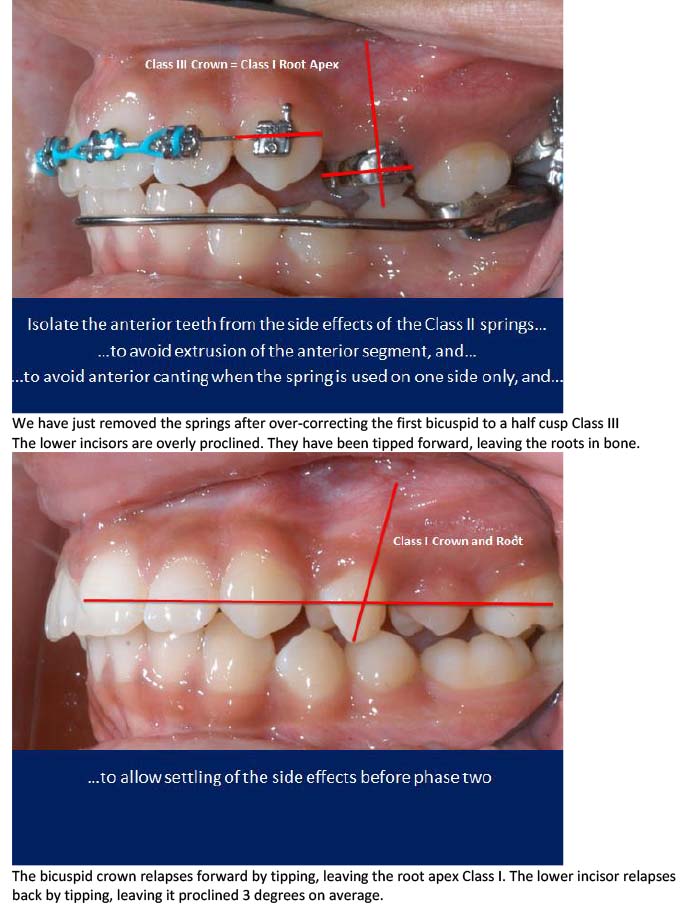
We have just removed the springs after over-correcting the first bicuspid to a half cusp Class III
The lower incisors are overly proclined. They have been tipped forward, leaving the roots in bone.

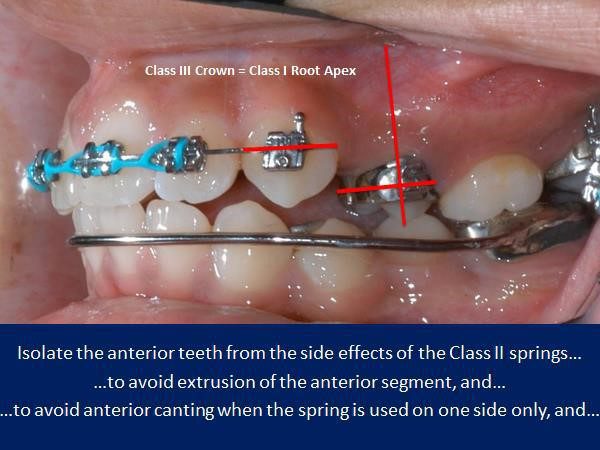
The bicuspid crown relapses forward by tipping, leaving the root apex Class I. The lower incisor relapses back by tipping, leaving it proclined 3 degrees on average.a
The greater the Class II, the greater the side effects from Class II elastics and Class II springs.
Class II elastics cause tooth eruption, which does not tend to relapse. Class II springs cause tooth intrusion and posterior open bite which does tend to relapse. Over-eruption of upper incisors (and upper canines with phase one Class II elastics) can lead to a gummy smile.
A unilateral Class II elastic on a full edgewise appliance (FEA) is no problem.
A unilateral phase one Class II elastic is likely to cause an occlusal cant that might be unrecoverable.
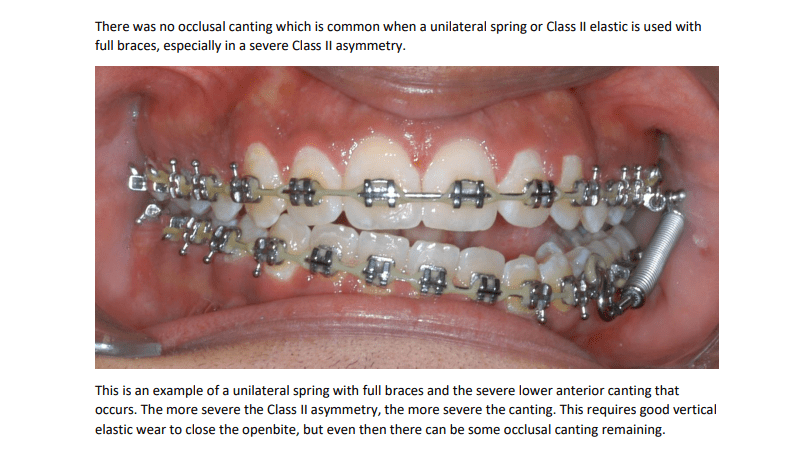
A unilateral Class II spring on an FEA can also cause an occlusal cant and an open bite that requires good anterior vertical elastic cooperation to resolve. A unilateral spring on an Xbow does not cause a cant because there are no brackets on the lower incisors. Any unilateral intrusion will relapse.
Class II springs with an FEA cause buccal flaring of upper molars, which may require posterior crossbite elastics to recover from. Class II springs on an Xbow do not cause the same flaring because of cross arch stabilization by the RME.
Both Class II elastics and Class II springs cause proclination of the lower incisors. Dr. Anthony Mair has warned about the use of Class II elastics with lower aligners, which cause bodily root movement, root prominence, and gingival recession of the lower incisors.
Xbow causes a temporary over-proclination of the lower incisors followed by partial but incomplete uprighting.
This is necessary in order to over-correct the Class II buccal relationship and to achieve the “bite-catching effect,” and a socked in Class I bicuspid relationship BILATERALLY!
The fact that the Xbow is a phase one appliance allows the clinician to achieve RAPID over-correction of the sagittal and transverse problems soon after the eruption of the first bicuspids to take advantage of the “bite-catching effect” of the steep cusps of the first bicuspids. The side effects such as posterior open bite and over-proclination of the lower incisors tend to relapse before phase two full edgewise.
The clinician has a better idea of where the incisors will end up after phase two and can modify the treatment plan at the beginning of phase two.
If there is still a deep overbite to treat in phase two, then a combination of a bite-turbo and Class II elastics maybe use for rapid bite-opening. The patient only has to cooperate with elastics for a short time so burnout is not as big a problem compared to depending on Class II elastic use in phase one and phase two to correct the entire malocclusion. There is also less chance of over-erupting the upper incisors with short term use of the Class II elastics.
Longer treatment time with Forsus to the archwire is due to dealing with the spring side effects late in treatment, such as posterior open bite and buccal flaring of the upper molars. The greater the correction, the greater the side effects, and the longer it takes to deal with them.
There is no buccal flaring of the upper molars with Xbow.
Much of the posterior open bite and proclination of the lower incisors rebound before full braces are placed.
Drs. Miller, Tieu, and Flores-Mir’s article titled “Incisor inclination changes produced by two compliance-free Class II correction protocols for the treatment of mild to moderate Class II malocclusions” is in the online version of the Angle Orthodontist.
It is based on Dr. Bob Miller’s clinical study.
He compared 36 Class II patients treated in one phase with Forsus to the archwire in a full edgewise appliance to 38 similar Class II patients treated in two phases with Xbow followed by a full edgewise appliance. The Forsus to the archwire group was finished in an average of 30.2 months (between records). The Xbow group was finished in an average of 24.2 months (between records), which included a 4 to 6 month rest period to allow for relapse. The two-phase Xbow patients were completed 6 months faster on average than the one phase Forsus to the archwire patients (time between records).
The Forsus to the archwire group had full braces for an average of 26.75 months. The Xbow group had full braces for an average of 16.68 months or 10 fewer months. There was no significant difference in the lower incisor to the mandibular plane angle between the two groups. The Xbow patients ended up with lower incisors at an average of 100 degrees to the mandibular plane, which is considered a reasonable compromise for non-extraction Class II compensation.
Editor’s note: Longer treatment time with Forsus to the archwire is due to dealing with the spring side effects late in treatment, such as posterior open bite and buccal flaring of the upper molars. The greater the correction, the greater the side effects, and the longer it takes to deal with them. There is no buccal flaring of the upper molars with Xbow.
Much of the posterior open bite and proclination of the lower incisors rebound before full braces are placed.

The side-effects of Forsus on the archwire are especially problematic when the spring is used unilaterally late in treatment.
The unilateral posterior openbite and anterior canting requires prolonged treatment with good elasitc cooperation to recover.
We do not see the anterior canting when the spring is used unilaterally on a Xbow because there are no lower brackets.
The fact that the first bicuspids are already Class I after Xbow therapy reduces the time in phase two braces and the need for side-effect correction with elastics.
I use the same principles when using the Forsus device with a full edgewise appliance as I do with Xbow.
Use the 22mm Direct Pushrod distal to the lower first bicuspid instead of the canine, if possible.
This keeps the Forsus device more compact and moves it distal to the anterior curvature of the arch, preventing the need for rod adjustments. It also keeps the spring distal to the Obicularis Oris muscle, preventing sores.
The only difference is you cannot fully compress the spring with an edgewise appliance if you use a bracket as the anterior stop.
If you do be prepared to rebond the bracket. Don’t forget to steel tie the first bicuspids.
Reactivate the springs with crimpable stops on the rods or use longer rods. Dr. Bob Miller taught us to hook up the pushrod using an Alastic KX module to activate the spring but at the same time remove the force from the canine or first bicuspid bracket. This also negates the need to cinch the distal end of the arch wire.
Place the springs and pushrods as you would normally but don’t close the loop yet. Make the pushrod adjustments leaving 1mm of play in the spring, remove the pushrod, pre-stretch a KX-1 module, place the KX module on the pushrod, place the pushrod on the archwire, close the pushrod loop, hook the KX module to the first molar hook using floss and a floss threader over the second bicuspid bracket and down between the second bicuspid and first molar, then place the pushrod in the spring. This completely activates the spring without debonding the canine or first bicuspid bracket.
If we place the 22 mm or 25 mm pushrod distal to the first bicuspid we use a KX-1 module.
We also use a KX-1 module distal to the canine in a bicuspid extraction case.

Alastic KX-1 module placed with floss threader

Alastic KX-1 module and lingual tuck-in pushrod adjustment on 25mm rod

Alastic KX-1 module hook-up distal to canine (severe Class II, patient decided against mandibular advancement surgery after preparation)

Alastic KX-1 Module hook-up distal to first bicuspid

Alastic KX-1 Module hook-up distal to canine (bicuspid extraction) with a 22 mm pushrod.

Spring Sleeve available from Comfort Solutions
Airway and XBOW®
Upper Airway Changes after Xbow Appliance Therapy Evaluated with CBCT Angle Orthodontist, Vol 84, No 4, 2014
Conclusions
1. Treatment with the Xbow appliance in Class II patients resulted in favorable dental and skeletal changes in the direction of a Class II correction.
2. An increase in the oropharyngeal airway dimensions and volume was observed in the cephalometric and three-dimensional evaluation of the upper airway.
There were no changes in the nasopharyngeal region and adenoid tissues.

Before


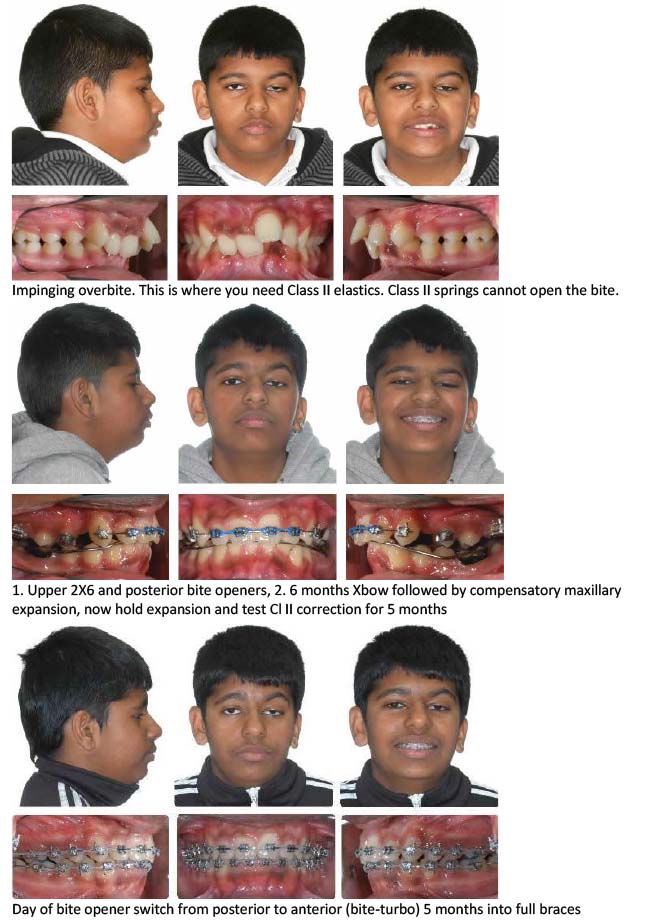
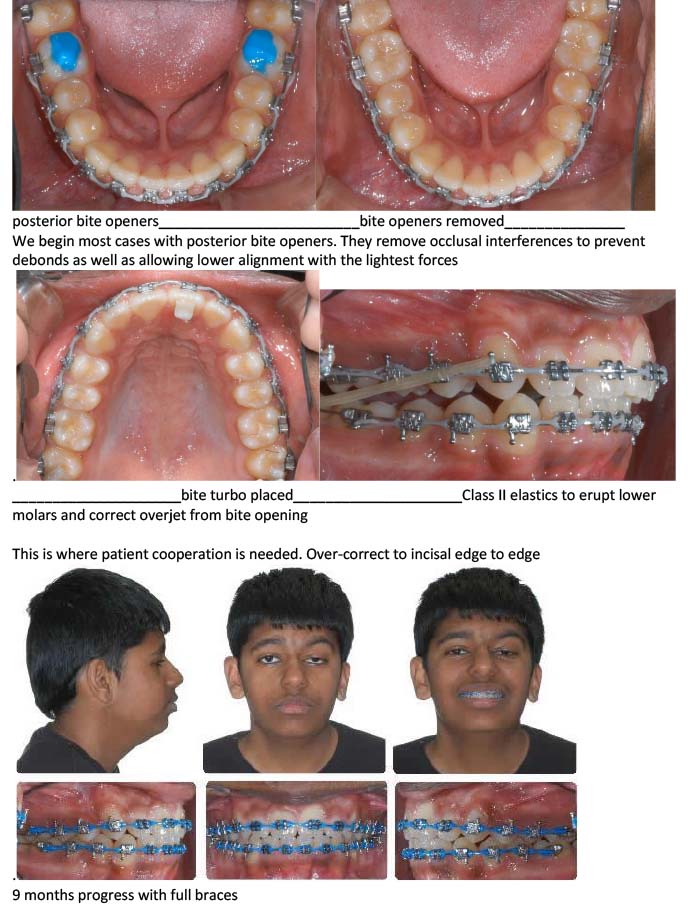
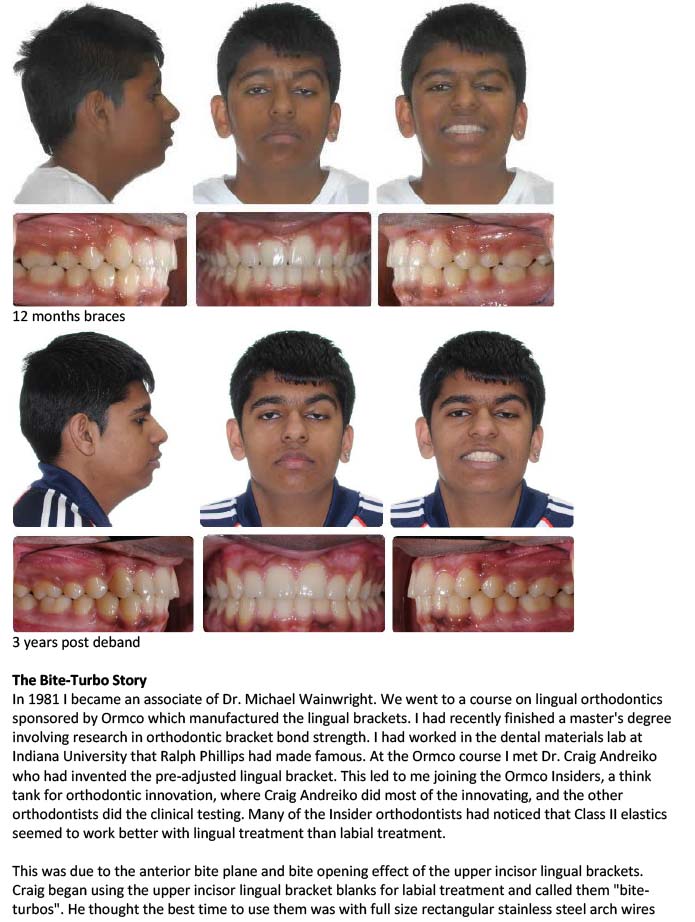
Class II Elastics vs Class II Springs


Impacted Canines: A Case for Crossbow

Unilateral Class II: A Case for Crossbow

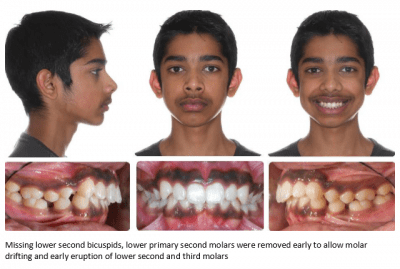
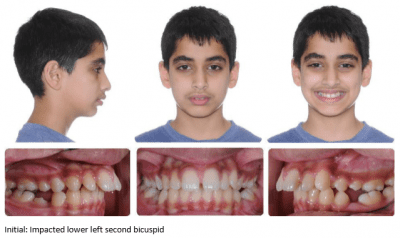
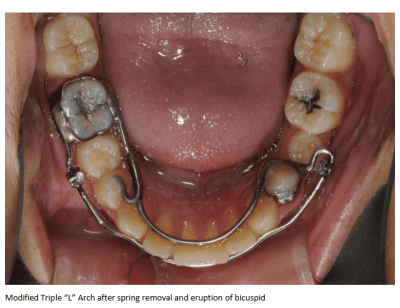
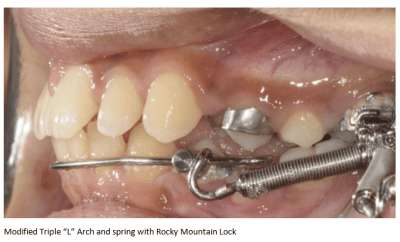
Impacted Lower Second Bicuspid: A Case for Crossbow
Missing Lower Second Bicuspids: A Case for Crossbow