Navigation
The Four Tool Boxes for Class II Treatment
Informed consent is the legal responsibility of the orthodontist to explain the pros and cons of all possible treatment options and to help the patient and their family determine which option is best for them.
One type of Class II bite problem is when there is a horizontal gap between the upper and lower front teeth, also known as excess overjet. 53% of the population has a Class II bite with an overjet greater than 3mm. 15% of the population has a moderate to severe Class II bite problem with 5mm or more of overjet.
The cause of excess overjet is usually a small or receding lower jaw and chin, but there can also be a protrusion of the upper front teeth.
Xbow System Lectures
Xbow Basics and Treated Cases

Xbow® (Crossbow) Class II Corrector
US Patent No. 6,168,430 B1
Canadian Patent No. 2,392,021


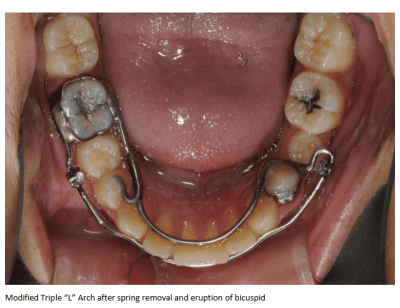
Triple “L” Arch® (Lower Labial Lingual)
Open Wide! (Pushrod Distalization)
Xbow (Crossbow)
- Cross or hybrid appliance
- Lower labial and lingual bow

3M Forsus Fatigue Resistant Device

Dr. Herb Hughes
Dr. Bob Miller

3D Metal Printing
(CAD-CAM,
Laser-Sintered Bands,
No-Separator Bands)


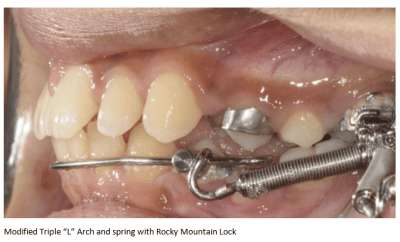
Large Rocky Mountain Lock

Rotated Over 180 Degrees

Xbow 5 months
Compensatory Maxillary Expansion 1 month + Retention 5 months
FEA 11 months


6+6+12=Blended Two Phase
- 4-6 months Class II springs on Xbow
- 1 month compensatory maxillary expansion + 5 months holding expansion = 6 months
- During expansion retention we test the Class II correction.
- Replace springs on one or both sides, if necessary
- R and R: Rebound and Periodontal Recovery
- Allow the Class II spring side effects to settle.
- 12 months phase two.
Two Phase Motto
- Only place full edgewise appliances on Class I buccal occlusions…
- after all permanent teeth have erupted, including second molars, and…
- with adequate maxillary width, and…
- with maxillary canines in place or at least adequate space for them.
RME X 6



Xbow + RME X 6


6 months

RME X 6
Xbow 4 months
FEA 9 months







Pancherz H. AM J ORTHOD. 1982;82:104-113
Xbow uses the same overcorrection and rebound as Herbst
Xbow’s Target:

Class I first bicuspid bilaterally in phase one


The Target is Class I Crowns and Roots


The Hughes Xbow Protocol
Dr. Herb Hughes
- Our normal protocol is to insert both portions of the Xbow, have the patient turn the screw 14-21 times, see them in 2-3 weeks and insert the springs. We can make transverse adjustments if needed throughout the Xbow time which is usually 5 to 6 months. Afterwards we remove the Xbow place fixed appliances along with bite ramps on the lingual of the upper 4’s (Dr. Shane Langley) to reinforce the Class I posterior relationship and open the bite if necessary to avoid bracket failure. Fixed appliances are usually on for months of time not years. Depending on the amount of crowding most cases are in fixed appliances for approximately 12 months.


3 months

5 months

6 months
Dr. Herb Hughes

6 months

10 months

Xbow: left spring 3 months, right spring 5 months
RME
Replace springs for 3 months

2 months after Xbow removal

FEA 14 months

5 years post deband

Xbow 4 months
RME
Replace springs 4 months
RME

6 months after spring removal.

FEA 8 months

2 years post deband

6 years post deband

Xbow 8 months


FEA 12 months

4 years post deband
Subdivision and Asymmetric Cases

RME X 4
Xbow with right spring 4 months


3 years post springs
Phase one only








Xbow
Left spring 3 months
Right spring 5 months


FEA 12 months

6 years post deband

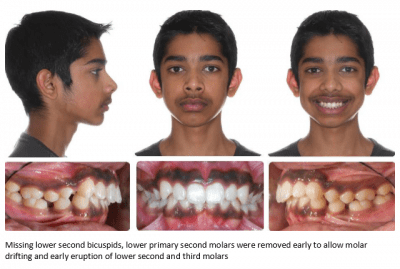
Missing lower second bicuspids
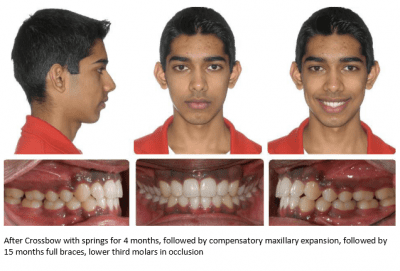
Xbow 4 months
RME

FEA 15 months
Phase One Only

Xbow 4.5 months
Compensatory Maxillary Expansion

3 months post springs

14 months post springs


RME X 4
Xbow 4 months
RME

Phase One Only

1. RMEX6 2. Xbow (springs for 3 months)

Phase one only

RME

RME X 6
Xbow left spring 3 months
RME

Phase One Only

1. RME 2. Xbow 3 months 3. RME

FEA 15 months

RME X 6
Xbow 4 months
RME


FEA 10 months

2 years post deband

Options
1. Mandibular Advancement Surgery
2. Extract upper first bicuspids and headgear
3. RME X 6, Xbow 5 months, FEA 14 months



History of Xbow
History and Rationale for Xbow: “Dealing With Side-Effects”
Class II Treatment History
- 1981, Wainwright, Hawley/headgear combination
- 1984, Frankel, Bionator/High-Pull Headgear
- 1990, Twin Block/High-Pull Headgear
- Poor compliance with headgear, elastics, and removable functional appliances.

- 1995, For large overjets: Four Crown Cantilever Herbst, treatment time in phase two reduced to 12 months with much fewer Class II elastics
- Subdivision cases were still a problem that required unilateral Class II elastics

- For mild to moderate Class II’s: Ormco Bite-Fixer Spring to the archwire (Low force, non-protrusive Jasper Jumper

- Advantage was the spring could be used unilaterally in asymmetric Class II’s, but the…
- Disadvantages were Class II correction wasn’t started until mid treatment…
- Which extended treatment time in full edgewise appliances compared to two phase treatment
Incisor inclination changes produced by two compliance-free Class II correction protocols for the treatment of mild to moderate Class II malocclusions.
Miller et al.
Angle Orthod 2013

Conclusions
- The Xbow two phase protocol averaged 6 fewer months of overall treatment and 10 fewer months of fixed edgewise appliances
compared to the Forsus to the archwire single phase protocol. (26.75 months for the Forsus to the archwire group vs 16.68 months for the
Xbow group) - No differences in incisor inclination between treatment protocols were identified.
- Lower incisors proclined more the longer the treatment.

- Waiting for second molars to erupt before beginning treatment and beginning Class II springs at 12 years or later could mean missing the growth spurt in early maturing females.
- Do we place FEA’s before second molars erupt and risk longer treatment, decalcification, root resorption, and burnout, or use two-phase treatment to catch growth?
Eruption Based Treatment Sequencing
- Half the battle is getting the brackets in the right place and using an efficient system of mechanics in phase two.
- The other half is what you do while you wait for the second molars to erupt, or…
- What you do between the time the maxillary first bicuspids and the second molars erupt.
Eruption Based Treatment Sequencing Pyramid

Class II Spring to the Archwire Side Effects
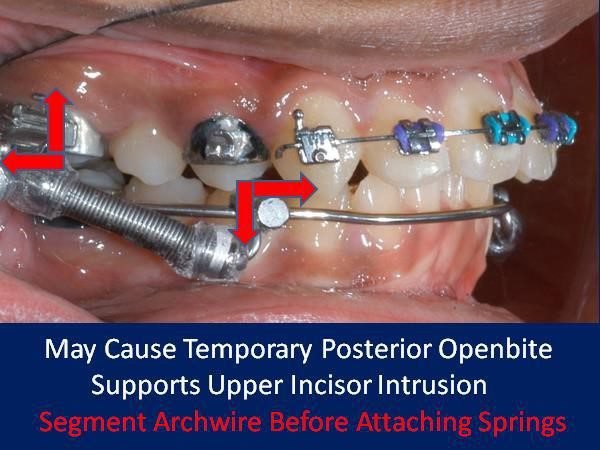
- Posterior openbite
- Buccal flaring of upper molars
- Proclination of lower incisors
- Anterior occlusal plane canting when used unilaterally

No incisor brackets to cause intrusion or occlusal canting.

Occlusal rests are added to the lower first bicuspids to direct the intrusive force to those teeth and to prevent the lingual and labial bows from impinging on the gingiva
Segment Archwire Before Attaching Springs

RME X 6/Xbow

Isolate the anterior teeth from the side effects of the Class II springs…
…to avoid extrusion of the anterior segment, and…
…to avoid anterior canting when the spring is used on one side only, and…

Lower Incisor Proclination
Controversies: Lower Incisor Proclination
Lower Incisor Inclination during Class II Malocclusion Treatment with the Xbow Appliance followed by Fixed Appliances
Fern Leavens (4th year dental student) Summer Research Project (2015) Under the supervision of Dr. Flores-Mir Unpublished
- 172 consecutively treated patients
- T1-T2 = phase one Xbow, T2-T3 = phase two full edgewise
- The mean lower incisor inclination changed from T1 (99.1o) to T2 (102.2o), with a mean difference of 3.1o. The change is statistically significant (p<0.001).
- The mean lower incisor inclination changed from T2 (102.2o) to T3 (103.7o), with a mean difference of 1.5o. The change is
statistically significant (p=0.01). This may not be clinically significant. - The mean lower incisor inclination changed from T1 (99.1o) to T3
(103.7o), with a mean difference of 4.6o. The change is statistically significant (p<0.001).
Prediction Equation for Lower Incisor Inclination Based on Initial Overbite
- Prediction equation is L1IncDiffT3 T1 = -2.2 + 1.3(OB). Or for every extra mm of OB (greater than the ideal overbite of 2mm) there is an increase in lower incisor inclination of 1.3o

Xbow 4 months
RME
10 months FEA


2 years post deband

History
- Proclination of lower incisors has been criticized since Angle.
- Calvin Case, who in the extraction debate with Angle in 1911, argued that proclination led to protrusive profiles, gingival recession, and unstable alignment leading to rapid relapse.
-
Tweed (1940) argued that the upright lower incisor seen in an ideal Class I skeletal pattern should be the goal in a Class II skeletal pattern for facial balance, stability, and periodontal health.
-
In most cases this required the removal of all first bicuspids due to lower crowding and lower mesialization due to Class II elastics.
- Casko (1984) argued that upright lower incisors were not the norm in an untreated Class II skeletal population. He said lower incisor proclination due to treatment copied “natural compensation in an untreated Class II skeletal population”.
Dental and Skeletal Variation Within the Range of Normal
JOHN S. CASKO, WALTER B. SHEPHERD
The Angle Orthodontist: 1984, Vol. 54, No. 1, pp. 5–17.
Untreated Class II and Class III Skeletal Sample with Ideal Occlusion (Naturally Compensated)

Pattern of Accommodation: “When the ANB angle is high, the mandibular plane angle is steeper, the cant of the occlusal plane is high and the incisors are more upright in the maxilla and more protrusive in the mandible.”

Herbst Appliance
- 1909: Herbst introduces the “rod and tube” fixed functional appliance
- 1979: Pancherz introduces the bonded cast framework Herbst appliance
- Tweed orthodontists criticized Pancherz for proclining lower incisors, and warned this would result in gingival recession.
- Pancherz added brackets to the lower inciosrs for torque control, called it the Edgewise Herbst.
- Instead of proclining lower incisors they were moved bodily, resulting in “washboard roots”.
Immediate Skeletal and Dentoalveolar Effects of the Crown- or Banded Type Herbst Appliance on Class II division 1 Malocclusion A Systematic Review
Barnett et al.
Angle Orthod 2008


All Class II elastics, springs, and functional appliances result in mesialization of the mandibular dentition
Bodily movement with torque control

Tipping to keep the roots in bone



Dr. Anthony Mair
Does orthodontic proclination of lower incisors in children and adolescents cause gingival recession?
S Ruf, K Hansen, H Pancherz
“No interrelation was found between the amount of incisor proclination
and the development of gingival recession.”
“This phenomenon may have been due to the fact that an approximately 80% spontaneous reversal of the incisor proclination after Herbst treatment occurs.”

July 1998 • Volume 114 • Number 1
- Proclined mandibular incisors rebounded in Herbst patients 32 years after therapy.
- Incisor irregularity increased, probably because of the physiologic processes occurring throughout life.
- Minor gingival recessions 32 years after treatment seemed unrelated to tooth inclination changes.
Orthodontic therapy and gingival recession: a systematic review
Prevalence of gingival recession after orthodontic tooth movements
Gingival recession in orthodontic patients 10 to 15 years posttreatment: A retrospective cohort study
- Prevalence of gingival recession increases during and after orthodontic treatment.
- Recession was similar in patients and untreated controls 15 years later.
- Orthodontic patients seem to not have worse long-term outcomes in regard to the prevalence of gingival recession than untreated controls seeking orthodontic treatment.
J. Periodontology June, 1981
- “gingival clefts were not seen after orthodontic therapy in any area that had even the smallest width of keratinized gingiva prior to orthodontic therapy.”
- “it is felt that a free gingival graft to create a new zone of keratinized gingiva should sometimes be performed prior to orthodontic therapy”
- “no correlation existed between the periodontal change and the change in angulation of the mandibular central incisors.
Functional appliances vs Xbow
Functional appliances vs Xbow
Functional Appliance Controversies
- Are we growing mandibles?
- Do fixed functionals work better than removables?
- Are there risks to forcing the condyle to function out of the fossa with Herbst?
- Or do the benefits to the airway outweigh the risks to the joint?
- Are the effects similar to Class II elastics?
- If that is the case, is a Herbst appliance like “taking a tank to the grocery store to buy a quart of milk”?
Twin-block vs Xbow
- Dental and skeletal changes in mild to moderate Class II malocclusions treated by either a Twin-block or Xbow appliance followed by full fixed orthodontic treatment. Sayeh Ehsani ; Brian Nebbe ; David Normando ; Manuel O. Lagravere ; Carlos Flores-Mir (Angle Orthod. 2015;85:997–1002.)
- As for mandibular changes, the corpus length increase was larger in the Twin-block group by 3.9 mm, but an improvement of sagittal position of pogonion was not detected.
Herbst vs Xbow
- Retrospective comparison of dental and skeletal effects in the treatment of Class II malocclusion between Herbst and Xbow appliances. Natalia Martins Insabralde, Marcio Rodrigues de Almeida, Renata Rodrigues de Almeida-Pedrin, Carlos Flores-Mir, and Jose Fernando Castanha Henriques (Am J Orthod Dentofacial Orthop 2021)
- a larger increase in mandibular length (an additional 3.2 mm) was noted for the Herbst group.
History
- DeVincenzo wrote the chapter on Class II correction and compliance in Graber and Swain and in 1997 developed the first telescopic spring, the “Eureka Spring”.

The analysis of the effect of treatment with functional appliances vs an untreated control group showed that skeletal changes were statistically significant, but unlikely to be clinically significant.
- Woodside and Harvold at the U of Toronto modified the Andresen activator which was worn part time, including nights.
- Woodside was critical of the Herbst appliance. His monkey studies showed that the condyles could remodel in both directions. The Herbst caused soft tissue stretching and condylar lengthening, but removal caused compression and condylar resorption.
- Woodside preferred the Crossbow appliance to the Herbst because it allowed the condyle to function in the fossa.
Dr. Don Woodside
- Warned that fixed functional appliances that forced the condyle to function out of the fossa may have negative effects on the TMJ.
- Thought it was safer to use removable functional appliances or light force, non-protrusive springs such as Forsus.
- Herbst appliances appear to achieve skeletal results by stretching the bilaminar retrodiskal elastic band between the condyle and the glenoid fossa. In contrast, chronic compression of the condyle produces severe condylar resorption that can be prevented to some extent with occlusal coverage by distracting the condyle vertically. The condyle is negatively affected by the return of anterior digastric muscle function and by perimandibular connection tissue pull in retention, seating the condyle posteriorly into the fossa.
Improved clinical use of Twin-block and Herbst as a result of radiating viscoelastic tissue forces on the condyle and fossa in treatment and long-term retention: Growth relativity
John C. Voudouris, Hon DDS, DOrth, MScDa, Mladen M. Kuftinec, DMD (Harv), DStom, ScDb
American Journal of Orthodontics and Dentofacial Orthopedics
Volume 117 Issue 3 Pages 247-266 (March 2000)
DOI: 10.1016/S0889-5406(00)70231-9

November 1998 • Volume 114 • Number 5
Long-term TMJ effects of Herbst treatment: A clinical and MRI study
Sabine Ruf, DDS, Dr med denta
Hans Pancherz, DDS, Odont Drb
Giessen, Germany
Am J Orthod Dentofacial Orthop 1998;114(5):475-83

Fig. 3. Parasagittal MRIs of 4 Herbst patients (cases 3, 6, 9, and 10) exhibiting moderate to severe signs and symptoms of TMD. (See Table I. Tracings are given next to each original image for better orientation. Dotted area represents a fibrotic adaptation of the
bilaminar zone.
Am J Orthod Dentofacial Orthop 1998;114(5):475-83
Signs and symptoms of TMJ disorders in adults after adolescent Herbst therapy: A 6-year and 32-year radiographic and clinical follow-up study Hans Pancherz; Hanna Salé; Krister Bjerklin
Angle Orthod (2015) 85 (5): 735–742.
Conclusions: This longitudinal very-long-term follow-up study after Herbst therapy revealed only minor problems from the TMJ. The TMJ findings 6 years and 32 years after Herbst treatment corresponded to those in the general population. Thus, in the very long term, the Herbst appliance does not appear to be harmful to the TMJ.
Class II Elastics vs Class II Springs
Class II Elastics vs Class II Springs
or
When to Pull vs When to Push
or
When to Extrude vs When to Intrude

RME X 6, posterior bite openers
Xbow 6 months

Day of spring removal
Begin compensatory maxillary expansion with RME




FEA 12 months

3 years post deband

Good For Bite Opening (Especially With a Turbo) May Cause Upper Incisor Extrusion Greater the Class II, Greater the Side Effects Mandibular growth counters downward and backward rotation

May cause temporary posterior openbite Supports upper incisor intrusion


Custom weld the tube to compensate for the bicuspid position Control the vertical position of the incisors

2. Xbow (Springs for 6 weeks)


Positioning the upper incisor to support the upper lip

2. Xbow (Springs for 6 weeks)
3. 14 months FEA


2. Xbow with left spring for 1 month, right spring for 3 months


The Class II Compensation Compromise
Robbing Peter to Pay Paul
Class II Compensation Compromise
- For non-surgical Class II compensation…
- …Interarch Class II mechanics share the correction between the upper and lower which helps avoid over-retraction of the upper incisor and lip.
- This is why the upper lip looks better in cases treated by functional appliances compared to pure upper incisor retraction (ie. extraction of upper first bicuspids backed up with headgear)
- We see similar results for all interarch Class II appliances, elastics, springs, removable functional, or fixed functional
- They all procline lower incisors.
- The differences are probably not clinically
significant. -
If it’s not surgery… it’s compensation
-
The greater the skeletal discrepancy and the more severe the malocclusion…
-
…The greater the Class II compensation…
-
…The greater the compromise of lower incisor proclination and upper incisor and upper lip retraction.
-
If you extract four bicuspids to avoid lower incisor proclination, the greater the upper incisor and upper lip retraction.
"If the only tool you have is a hammer, every problem looks like a nail"

Our hammer is upper incisor retraction, even when the problem is almost always mandibular retrusion.
Drs. M Stoner and J Lindquist
- 1956: Angle Orthodontist; Consecutive Cases Treated by Dr. Charles Tweed
- Looked at the claim that Tweed mechanics resulted in improved facial esthetics.
- Most of the overjet correction was by upper incisor retraction.
- Dental compensation for a largely orthopedic problem
History
- Obwegeser, 1953: BSSO, 1970: simultaneous Le Fort 1 and BSSO
- Epker, 1979: modified the BSSO, described pre-surgical decompensation, extracting in the lower arch in Class II’s and in the upper arch in Class III’s, proclining lower incisors in Class III’s and upper incisors in Class II div 2’s.
- Epker would treatment plan by placing the upper incisor ideally in the face.
- This may require two jaw surgery.
- At the same time orthodontists were trained to treat to the lower incisor.
- Epker criticized upper incisor retraction in patients with mandibular retrognathia
- He also criticized functional appliances and early treatment for compromising an ideal surgical result.

Treatment plan: extraction of two lower bicuspids and mandibular advancement surgery

Surgery by Dr. Bill McDonald
Maxillary Expansion
Maxillary Expansion
- Cornerstone of Class II treatment, non-extraction treatment, minimizing buccal corridors, upper airway management
- 34-38mm inter-first molar palatal width
- Over-correction followed by lingual tipping of upper first molars results in correct buccal root torque
- Archwire expansion may result in insufficient buccal root torque on upper molars
- Hyrax RME is the backbone of Xbow

Superscrew



Crossbow's Competition
Crossbow's Competition
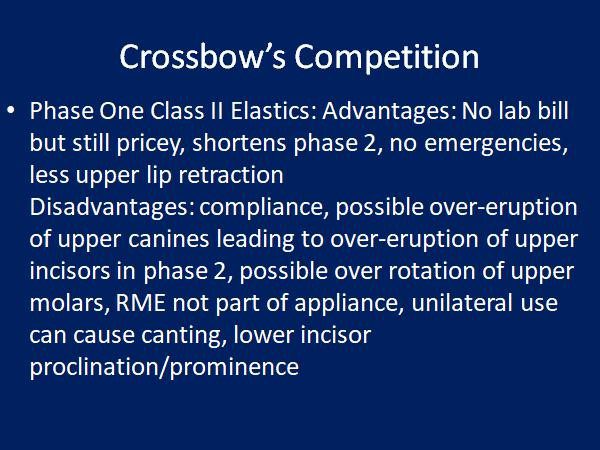
- Headgear: Advantages: easy to install, low cost, no lower incisor proclination, opens space for upper canines, no emergencies
Disadvantages: compliance, U7 impaction, upper lip retraction, not great for subdiv cases - Class II elastics: Advantages: low cost, best for lower molar eruption in deep overbite and short lower facial height, no emergencies, good for subdiv cases, less upper lip retraction.
Disadvantages: compliance, upper incisor eruption, lower incisor procliation/root prominence - Carriere Motion: Advantages: No lab bill but still pricey, shortens phase 2, no emergencies, less upper lip retraction
Disadvantages: compliance, possible over-eruption of upper canines leading to over-eruption of upper incisors in phase 2, RME not part of appliance, unilateral use can cause canting, possible lower incisor root prominence when used with lower Essix. - Twin Block: Advantages: two impressions, no emergencies, 1-2 mm extra mandibular length.
Disadvantages: compliance, speech, breakage, no banded RME, not great in subdiv cases, lower incisor proclination/prominence, needs overjet, not great with crowded upper canines - Herbst: Advantages: compliance, 1-2mm extra mandibular length, RME can be built in
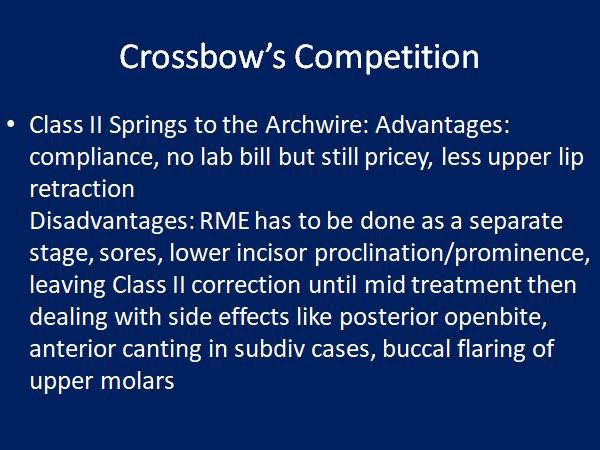
Disadvantages: lab bill, crowns hard to remove, needs overjet, not great with crowded upper canines, sores, lower incisor proclination/prominence, not great in subdiv cases - Class II Springs to the Archwire: Advantages: compliance, no lab bill but still pricey, less upper lip retraction
Disadvantages: RME has to be done as a separate stage, sores, lower incisor proclination/prominence, leaving Class II correction until mid treatment then dealing with side effects like posterior openbite, anterior canting in subdiv cases, buccal flaring of upper molars, late treatment may miss growth spurt in early maturing females. - Crossbow: Advantages: compliance, unilateral control similar to Class II elastics, RME built in, LLA built in, RME X 6 compatible, opens space for U3’s, side effects settle before phase 2
Disadvantages: cost, 6 bands, proclines lower incisors, sores, pushrod adjustment
The Four Tool Boxes for Class II Treatment
The Four Tool Boxes for Class II Treatment
Informed consent is the legal responsibility of the orthodontist to explain the pros and cons of all possible treatment options and to help the patient and their family determine which option is best for them.
One type of Class II bite problem is when there is a horizontal gap between the upper and lower front teeth, also known as excess overjet. 53% of the population has a Class II bite with an overjet greater than 3mm. 15% of the population has a moderate to severe Class II bite problem with 5mm or more of overjet.
The cause of excess overjet is usually a small or receding lower jaw and chin, but there can also be a protrusion of the upper front teeth.
The Four Tool Boxes Analogy
Dr. Higgins’ office has four different options for treating a Class II bite problem.
- The Surgery Tool Box
Braces to straighten the teeth and place the front teeth and lips in an ideal position, followed by surgery to lengthen the lower jaw, is often the best option to correct the bite and balance the appearance of the nose, lips, and chin. - The Traditional Treatment Tool Box
Braces and the extraction of two upper teeth are used to retract or “pull back” the upper front teeth to correct the bite and camouflage the small or receding lower jaw and chin. We call this Class II compensation. This is a good choice if the upper front teeth are crowded or protruding. The downside of this treatment is that it can result in the loss of upper lip fullness. - The Crossbow Tool Box
The Crossbow Class II Corrector shares the correction between the upper and lower teeth. It moves upper teeth back and lower teeth forward. This minimizes the retraction of the upper front teeth and upper lip. This is another type of Class II compensation. It is meant to be used in a growing patient and works best if the patient has a growth spurt. The downside is that it still moves the upper lip back, just not as much as traditional extraction treatment. It also moves the lower lip forward, a plus or a minus. Even if surgery is the best option, most patients still choose the Crossbow Tool Box to avoid surgery and extractions. Sometimes, the Crossbow is not a good option, especially if the patient is finished growing, if the lower front teeth are crowded or protruded, or if the lower lip protruded. - The Class II Elastic Tool Box
Combined with Class II elastics, braces or Aligners are probably the most common treatments today. It is popular because it is the least expensive. It requires the least effort by the orthodontist, but the most effort by the patient. If the patient does not wear the elastics, they end up with straight teeth but with a remaining bite problem or excess overjet.
If the patient wears the elastics well, the result may be similar to the Crossbow, with two exceptions. Class II elastics tend to pull the upper front teeth down, making a gummy smile worse. Two, when used with aligners, Class II elastics may push the lower front teeth out of the bone, exposing the roots. The other problem with aligners is they require much more patient cooperation than braces, and there are many tooth movements that aligners don’t do well or not at all.
This is why the best orthodontists using aligners use them with braces. Braces are still used to do the “heavy lifting.”The general rule is it is best to choose a treatment plan that decreases elastic wear and patient cooperation because poor cooperation can increase the length of treatment. Long treatment time increases the risk of root resorption (root shortening) and decalcification (white spot lesions or cavities).
Dr. Higgins has developed systems that decrease the time in braces to 12 to 18 months, even for extraction treatment. This includes indirect (precision) bonding of brackets (braces). He also uses a low-force technique with a smaller bracket slot and smaller wires than most orthodontists. This is more comfortable for the patients and may result in less root resorption.
The Crossbow appliance is part of Dr. Higgins’ “foundation building” treatment philosophy. It is based on waiting until all teeth have erupted, including second molars, before placing full braces. “Building the foundation” includes establishing a normal upper jaw width with an expander (RME), correcting a Class II bite with a Crossbow appliance, and opening space for upper canine teeth with partial braces (RME X 6).
Dr. Higgins is a clinical assistant professor at the University of British Columbia. More information can be found on the Crossbow website at www.crossboworthodontic.com.
(CAAPP) Orthodontic Skating: Sliding with Control
(CAAPP) Orthodontic Skating: Sliding with Control

CAAPP with G&H Agility PSL brackets on canines and bicuspids.
Combination Active Anteriors and Passive Posteriors (CAAPP) Orthodontic Skating: Sliding with Control
CAAPP with G&H Agility PSL brackets on canines and bicuspids.
CAAPP combines incisor control with ligated twin brackets and decreased resistance to sliding with passive self-ligating brackets on canines and bicuspids, creating a “long buccal tube.” Ligated incisors also give young patients what they ask for, such as colored ligatures.
.018 inch bracket slot, .018X.025 inch archwire, Carriere passive self-ligating bracket sliding on archwire with Innovation active self-ligating brackets acting as end stops.
.018 inch bracket slot, .016X.022 inch archwire, Lotus Plus passive self-ligating bracket sliding on archwire with Lotus Plus interactive self-ligating brackets acting as end stops.
In a group of 145 consecutively debonded patients from the author’s practice, the average treatment time from bonding to debonding was 16 months. 78% of the patients had an average treatment time of 13.4 months.
The part of treatment that the orthodontist has control over (other than the treatment plan) is Alignment and Space Closure (ASC). The patient controls elastic wear to coordinate the arches and finish the occlusion. In a group of 42 consecutively treated patients, where 34 were non-extraction, and 8 were extraction cases, ASC took an average of 9 months to complete for the non-extraction group and 11 months for the extraction group.
CAAPP TwinLok 1997
I was asked to test the .018 version of the TwinLok passive self-ligating bracket in 1997. The result was the incomplete alignment of the lower incisors and a lack of torque control of the upper incisors. This was due to the play between the archwire and the slot. The slot depth was .030 inches. This was done to accommodate the anterior curvature of the archwire and still allow the clips to close.
The low resistance to sliding in the canine and bicuspid brackets was an advantage. It was easier to close space, retract canines, and advance incisors.
I changed the TwinLok brackets to ligated twins on the incisors and traded free sliding for control, creating a hybrid system similar to Dr. Gianelly’s bi-metric technique.
Ligating the archwire to the incisor bracket slots’ base allows the maximum deflection and activation of the lightest archwires and the fastest incisor alignment with the lightest forces.
Proponents of passive self-ligating brackets thought that ligated incisor brackets would slow down anterior alignment and require heavier forces to overcome resistance to sliding. The following examples show that this is not the case.



Initial




The following is a bicuspid extraction case showing rapid alignment with CAAPP.

Initial




I am using the Lotus Plus DS Hybrid self-ligating bracket system, which is active on incisors and passive on canines and bicuspids. I use the MBT prescription in a .018-inch slot. The slot tolerances are tight, and we sometimes find it difficult to close the clips when using .017X.025-inch archwires.
Presently, the archwire progression we are using is .012-inch niti, followed by .014-inch niti (if necessary), followed by .018-inch niti to the second molars, followed by .016X.022-inch niti, and finally, .017X.022-inch heat-treated stainless-steel archwires. Final adjustments are done in .016X.022-inch beta titanium.
When I started with Dr. Michael Wainwright, he used two archwires, a .016-inch Niti followed by .016X.022-inch stainless steel. I was amazed at the simplicity and efficiency compared to the segmented arch technique that we were both taught at Indiana University. I am now using more archwires in the progression, but I am convinced I am using the lightest forces, decreasing root resorption and making it more comfortable for my patients.


The Lotus Interactive Niti clip seats the archwire in the slot’s floor with a force perpendicular to the slot, unlike a “C” Clip.

Four arch sizes=three pairs (Small, Medium, Large)
To purchase these wires in most sizes contact Mark James at G and H Orthodontics.
Crossbow's Competition and Dealing With Side Effects

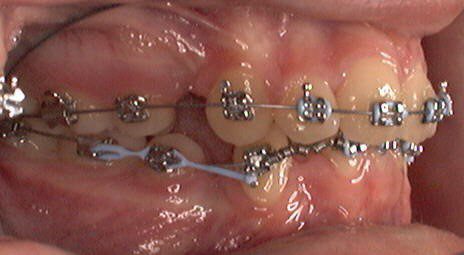
Bite opening in phase two with eruption mechanics (bite turbo and Class II elastics) while the patient is growing and mandibular growth can compensate for the downward and backward rotation of the mandible.


Initial unilateral Class II

Left spring only

Over-correction after 5 months, incisors edge to edge, note side effect of posterior openbite but no anterior occlusal canting

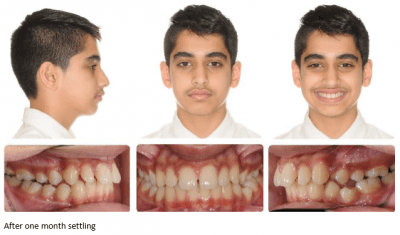
After 1 month settling

After 2 months settling

After 5 months settling

This is an example of why we segment the arch wire distal to the canine before placing springs.
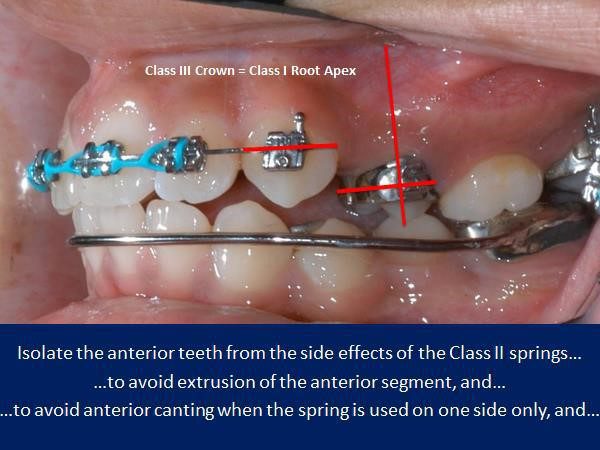
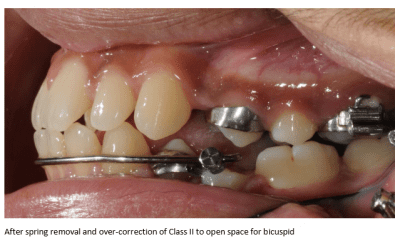
We have just removed the springs after over-correcting the first bicuspid to a half cusp Class III
The lower incisors are overly proclined. They have been tipped forward, leaving the roots in bone.

The bicuspid crown relapses forward by tipping, leaving the root apex Class I. The lower incisor relapses back by tipping, leaving it proclined 3 degrees on average.a
The greater the Class II, the greater the side effects from Class II elastics and Class II springs.
Class II elastics cause tooth eruption, which does not tend to relapse. Class II springs cause tooth intrusion and posterior open bite which does tend to relapse. Over-eruption of upper incisors (and upper canines with phase one Class II elastics) can lead to a gummy smile.
A unilateral Class II elastic on a full edgewise appliance (FEA) is no problem.
A unilateral phase one Class II elastic is likely to cause an occlusal cant that might be unrecoverable.
A unilateral Class II spring on an FEA can also cause an occlusal cant and an open bite that requires good anterior vertical elastic cooperation to resolve. A unilateral spring on an Xbow does not cause a cant because there are no brackets on the lower incisors. Any unilateral intrusion will relapse.
Class II springs with an FEA cause buccal flaring of upper molars, which may require posterior crossbite elastics to recover from. Class II springs on an Xbow do not cause the same flaring because of cross arch stabilization by the RME.
Both Class II elastics and Class II springs cause proclination of the lower incisors. Dr. Anthony Mair has warned about the use of Class II elastics with lower aligners, which cause bodily root movement, root prominence, and gingival recession of the lower incisors.
Xbow causes a temporary over-proclination of the lower incisors followed by partial but incomplete uprighting.
This is necessary in order to over-correct the Class II buccal relationship and to achieve the “bite-catching effect,” and a socked in Class I bicuspid relationship BILATERALLY!
The fact that the Xbow is a phase one appliance allows the clinician to achieve RAPID over-correction of the sagittal and transverse problems soon after the eruption of the first bicuspids to take advantage of the “bite-catching effect” of the steep cusps of the first bicuspids. The side effects such as posterior open bite and over-proclination of the lower incisors tend to relapse before phase two full edgewise.
The clinician has a better idea of where the incisors will end up after phase two and can modify the treatment plan at the beginning of phase two.
If there is still a deep overbite to treat in phase two, then a combination of a bite-turbo and Class II elastics maybe use for rapid bite-opening. The patient only has to cooperate with elastics for a short time so burnout is not as big a problem compared to depending on Class II elastic use in phase one and phase two to correct the entire malocclusion. There is also less chance of over-erupting the upper incisors with short term use of the Class II elastics.
Longer treatment time with Forsus to the archwire is due to dealing with the spring side effects late in treatment, such as posterior open bite and buccal flaring of the upper molars. The greater the correction, the greater the side effects, and the longer it takes to deal with them.
There is no buccal flaring of the upper molars with Xbow.
Much of the posterior open bite and proclination of the lower incisors rebound before full braces are placed.
Drs. Miller, Tieu, and Flores-Mir’s article titled “Incisor inclination changes produced by two compliance-free Class II correction protocols for the treatment of mild to moderate Class II malocclusions” is in the online version of the Angle Orthodontist.
It is based on Dr. Bob Miller’s clinical study.
He compared 36 Class II patients treated in one phase with Forsus to the archwire in a full edgewise appliance to 38 similar Class II patients treated in two phases with Xbow followed by a full edgewise appliance. The Forsus to the archwire group was finished in an average of 30.2 months (between records). The Xbow group was finished in an average of 24.2 months (between records), which included a 4 to 6 month rest period to allow for relapse. The two-phase Xbow patients were completed 6 months faster on average than the one phase Forsus to the archwire patients (time between records).
The Forsus to the archwire group had full braces for an average of 26.75 months. The Xbow group had full braces for an average of 16.68 months or 10 fewer months. There was no significant difference in the lower incisor to the mandibular plane angle between the two groups. The Xbow patients ended up with lower incisors at an average of 100 degrees to the mandibular plane, which is considered a reasonable compromise for non-extraction Class II compensation.
Editor’s note: Longer treatment time with Forsus to the archwire is due to dealing with the spring side effects late in treatment, such as posterior open bite and buccal flaring of the upper molars. The greater the correction, the greater the side effects, and the longer it takes to deal with them. There is no buccal flaring of the upper molars with Xbow.
Much of the posterior open bite and proclination of the lower incisors rebound before full braces are placed.

The side-effects of Forsus on the archwire are especially problematic when the spring is used unilaterally late in treatment.
The unilateral posterior openbite and anterior canting requires prolonged treatment with good elasitc cooperation to recover.
We do not see the anterior canting when the spring is used unilaterally on a Xbow because there are no lower brackets.
The fact that the first bicuspids are already Class I after Xbow therapy reduces the time in phase two braces and the need for side-effect correction with elastics.
I use the same principles when using the Forsus device with a full edgewise appliance as I do with Xbow.
Use the 22mm Direct Pushrod distal to the lower first bicuspid instead of the canine, if possible.
This keeps the Forsus device more compact and moves it distal to the anterior curvature of the arch, preventing the need for rod adjustments. It also keeps the spring distal to the Obicularis Oris muscle, preventing sores.
The only difference is you cannot fully compress the spring with an edgewise appliance if you use a bracket as the anterior stop.
If you do be prepared to rebond the bracket. Don’t forget to steel tie the first bicuspids.
Reactivate the springs with crimpable stops on the rods or use longer rods. Dr. Bob Miller taught us to hook up the pushrod using an Alastic KX module to activate the spring but at the same time remove the force from the canine or first bicuspid bracket. This also negates the need to cinch the distal end of the arch wire.
Place the springs and pushrods as you would normally but don’t close the loop yet. Make the pushrod adjustments leaving 1mm of play in the spring, remove the pushrod, pre-stretch a KX-1 module, place the KX module on the pushrod, place the pushrod on the archwire, close the pushrod loop, hook the KX module to the first molar hook using floss and a floss threader over the second bicuspid bracket and down between the second bicuspid and first molar, then place the pushrod in the spring. This completely activates the spring without debonding the canine or first bicuspid bracket.
If we place the 22 mm or 25 mm pushrod distal to the first bicuspid we use a KX-1 module.
We also use a KX-1 module distal to the canine in a bicuspid extraction case.

Alastic KX-1 module placed with floss threader

Alastic KX-1 module and lingual tuck-in pushrod adjustment on 25mm rod

Alastic KX-1 module hook-up distal to canine (severe Class II, patient decided against mandibular advancement surgery after preparation)

Alastic KX-1 Module hook-up distal to first bicuspid

Alastic KX-1 Module hook-up distal to canine (bicuspid extraction) with a 22 mm pushrod.

Spring Sleeve available from Comfort Solutions
Airway and XBOW®
Upper Airway Changes after Xbow Appliance Therapy Evaluated with CBCT Angle Orthodontist, Vol 84, No 4, 2014
Conclusions
1. Treatment with the Xbow appliance in Class II patients resulted in favorable dental and skeletal changes in the direction of a Class II correction.
2. An increase in the oropharyngeal airway dimensions and volume was observed in the cephalometric and three-dimensional evaluation of the upper airway.
There were no changes in the nasopharyngeal region and adenoid tissues.

Before


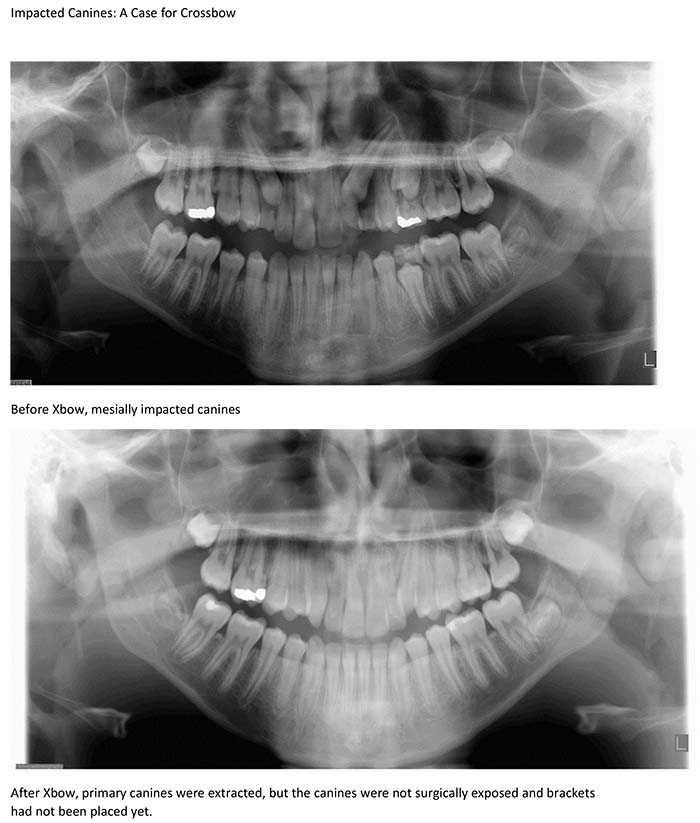
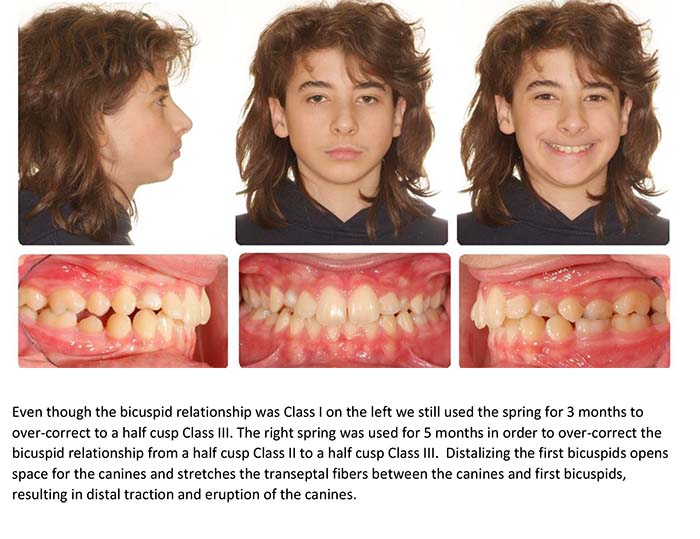
Impacted Canines: A Case for Crossbow

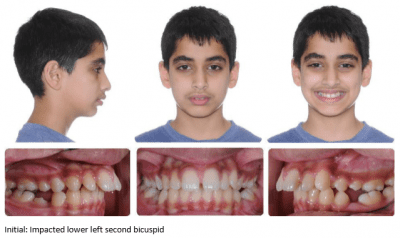
Impacted Lower Second Bicuspid: A Case for Crossbow
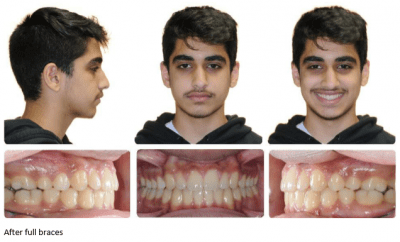
Missing Lower Second Bicuspids: A Case for Crossbow

Published Xbow Articles
"Short-term skeletal and dental effects of the Xbow appliance as measured on lateral cephalograms."As seen in the December 2009 American Journal of Orthodontics and Dentofacial Orthopedics.
As seen in the November 2010 Angle Orthodontist.
As seen in the October 2011 Angle Orthodontist.
“Drs. Flores-Mir, McGrath, Heo, & Major’s ‘Efficiency of Molar Distalization with the Xbow Appliance Related to Second Molar Eruption Stage’”
As seen in the November 2012 European Journal of Orthodontics.
As seen in the May 2013 Angle Orthodontist
As seen in the July 2014 Angle Orthodontist
“External Apical Root Resorption Generated by Forsus Simultaneously with Brackets vs. Xbow Followed by Brackets to Correct Class II Malocclusions”
As seen in the September 2015 Journal of the World Federation of Orthodontists
As seen in the November 2015 Angle Orthodontist
Dr. Bob Miller also compared eight two-phase Herbst cases with seven two-phase Xbow cases and seven single-phase Forsus cases.
Avg # of Visits
Herbst (two-phase) 29
Xbow (two-phase) 19
Forsus on archwire (single phase) 26
Avg Chair Time (min/visit)
Xbow (two-phase) 26
Forsus on archwire (single phase) 32
Avg Time in Office (min)
Xbow (two-phase) 556
Forsus on archwire (single phase) 818